
Respiratory System Drugs — MCQs

On this page
Which drug used in bronchial asthma requires therapeutic drug monitoring?
What is the therapeutic blood range of theophylline in micrograms per liter?
Which of the following drugs can be administered by the subcutaneous route?
Which of the following constituents of commonly used metered dose inhalers in bronchial asthma is also an air pollutant dangerous to the Earth's stratosphere?
A woman taking cetirizine for allergic rhinitis complains of excessive sleepiness. Which of the following is the best alternative with minimal sedative effect?
Benralizumab acts on which receptor?
The image given below shows a portable battery device called vibrating-mesh nebulizer for salbutamol delivery. All are correct about the device except:
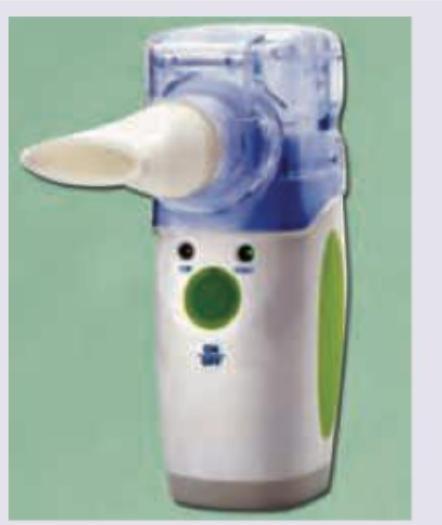
Which of the following instructions is not given if a second puff is required from this device?
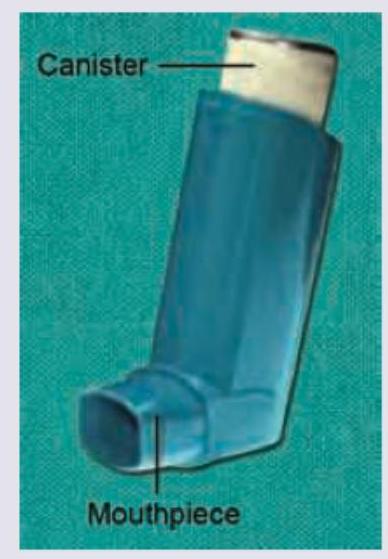
Consider the following steps for using a metered dose inhaler (MDI) : I. Incline the head backward to minimize oropharyngeal deposition II. Remove the cap and shake the inhaler III. Breathe out gently and place the mouthpiece into the mouth IV. Hold the breath for 10 seconds V. Simultaneously, begin a slow deep inspiration, depress the canister and continue to inhale Which one of the following is the correct sequence of using MDI?
Which of the following is a centrally acting non-opioid antitussive?
Practice by Chapter
Bronchodilators
Practice Questions
Corticosteroids in Respiratory Disorders
Practice Questions
Anti-inflammatory Respiratory Agents
Practice Questions
Mast Cell Stabilizers
Practice Questions
Leukotriene Modifiers
Practice Questions
Antitussives and Expectorants
Practice Questions
Nasal Decongestants
Practice Questions
Pulmonary Surfactants
Practice Questions
Drugs for Pulmonary Hypertension
Practice Questions
Oxygen Therapy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app