
Hospital Acquired Infections — MCQs

On this page
A 60-year-old nursing home resident presents with a 3-day history of progressive shortness of breath and cough. The lung examination reveals right basilar crackles. The chest x-ray shows right lower lobe consolidation. Sputum culture grows methicillin-resistant Staphylococcus aureus (MRSA). Select the most appropriate isolation precaution.
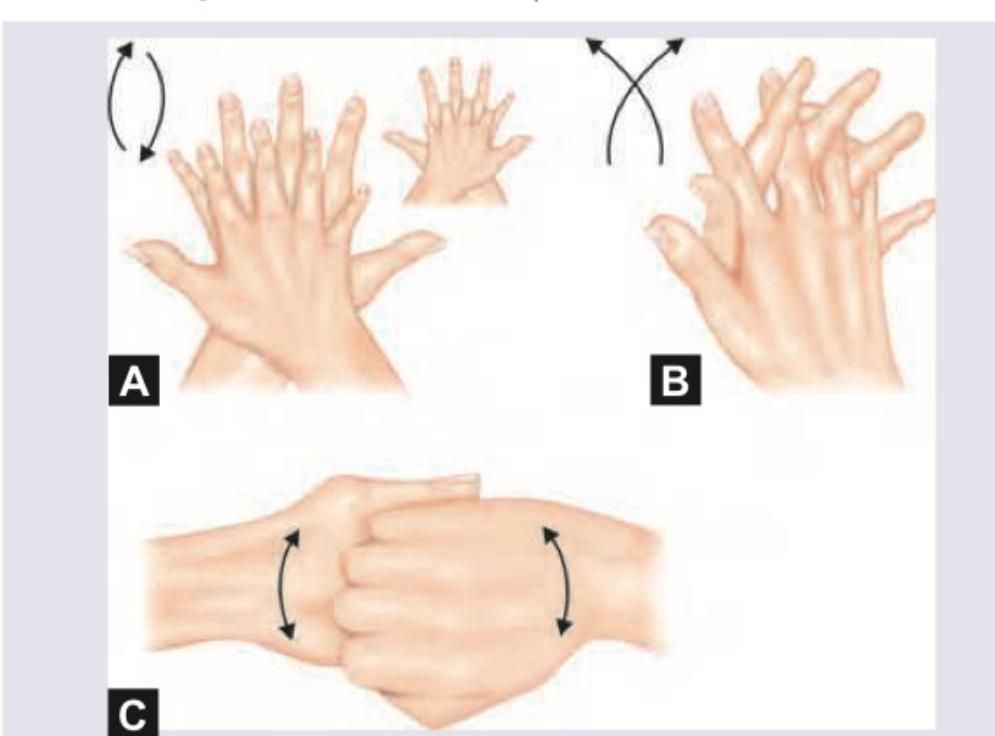
Which is correct sequence of handwashing technique?
An 18-year-old college student presents with fever, headache, neck stiffness, and petechial rash on his ankles. Lumbar puncture shows abundance of white blood cells with extracellular as well as intracellular gram-negative diplococci. Select the most appropriate isolation precaution.
In which body site do health workers commonly carry microbes causing healthcare-associated infections (haemolytic Streptococcus)?
Not a cause of community acquired pneumonia -
A patient in ICU and on ventilator develops cough with fever. The gram-staining on microscopy will show:
Best method of preventing transmission of MRSA infection is
A common source of Staphylococcus in the hospital is:
A study of nosocomial infections involving urinary catheters is performed. The study shows that the longer an indwelling urinary catheter remains, the higher the rate of symptomatic urinary tract infections (UTIs). Most of these infections are bacterial. Which of the following properties of these bacteria increase the risk for nosocomial UTIs?
Hospital-acquired organisms include all except?
Practice by Chapter
Epidemiology of Hospital Infections
Practice Questions
Catheter-Associated Urinary Tract Infections
Practice Questions
Ventilator-Associated Pneumonia
Practice Questions
Surgical Site Infections
Practice Questions
Central Line-Associated Bloodstream Infections
Practice Questions
Clostridium difficile Infection
Practice Questions
Hospital Infection Control Programs
Practice Questions
Isolation Precautions
Practice Questions
Hand Hygiene
Practice Questions
Environmental Cleaning and Disinfection
Practice Questions
Surveillance of Hospital Infections
Practice Questions
Bundle Approach to Prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app