
Diagnostic Microbiology — MCQs

On this page
Acridine orange is a fluorescent dye used to bind which cellular components?
What is the investigation of choice for detecting syphilis in a patient after two courses of complete therapy?
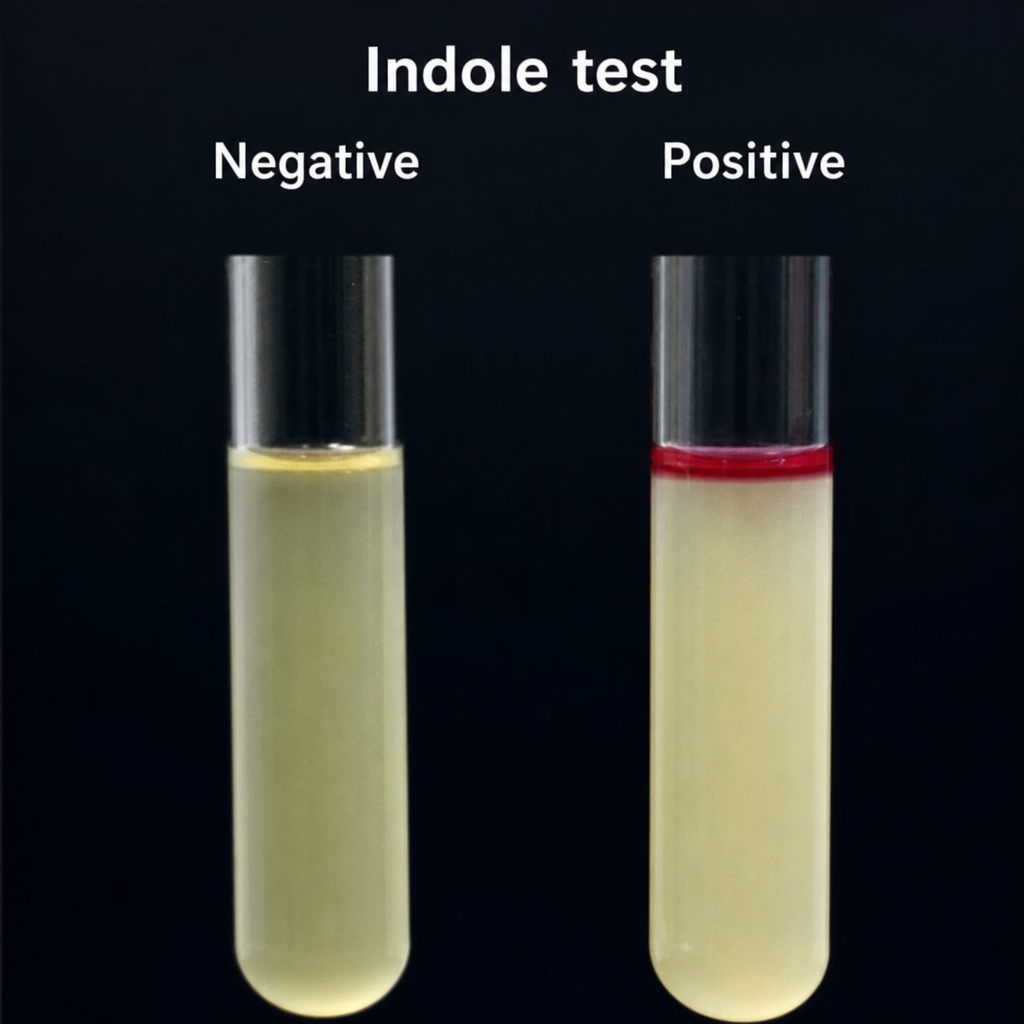
Which of the following bacteria shows this test positive?
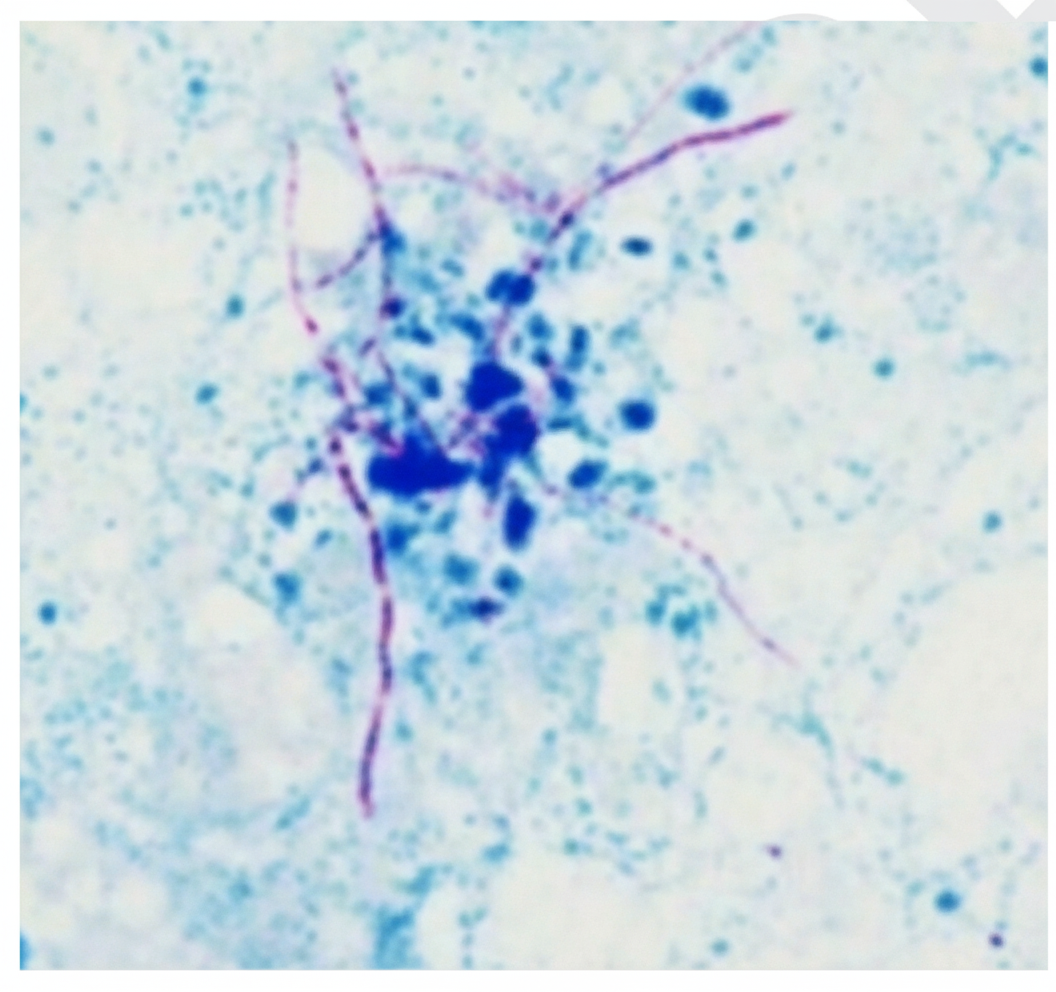
What is the staining technique used here?
Which of the following methods does not establish the diagnosis of congenital Cytomegalovirus (CMV) infection in a neonate?
Which of the following are non-invasive tests for Helicobacter pylori?
The tuberculin test is associated with all of the following findings except:
Which is the most sensitive test for HIV infection?
Which specific test is used for the diagnosis of Treponema pallidum infection?
What is the culture media of choice for growing most fungi?
Practice by Chapter
Specimen Collection and Transport
Practice Questions
Microscopy in Microbiology
Practice Questions
Culture Methods and Media
Practice Questions
Bacterial Identification Techniques
Practice Questions
Antimicrobial Susceptibility Testing
Practice Questions
Serological Diagnosis
Practice Questions
Molecular Diagnostic Methods
Practice Questions
Rapid Diagnostic Tests
Practice Questions
Point-of-Care Testing
Practice Questions
Automation in Microbiology Laboratory
Practice Questions
Quality Control in Diagnostic Microbiology
Practice Questions
Interpretation of Microbiological Reports
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app