
Diagnostic Microbiology — MCQs

On this page
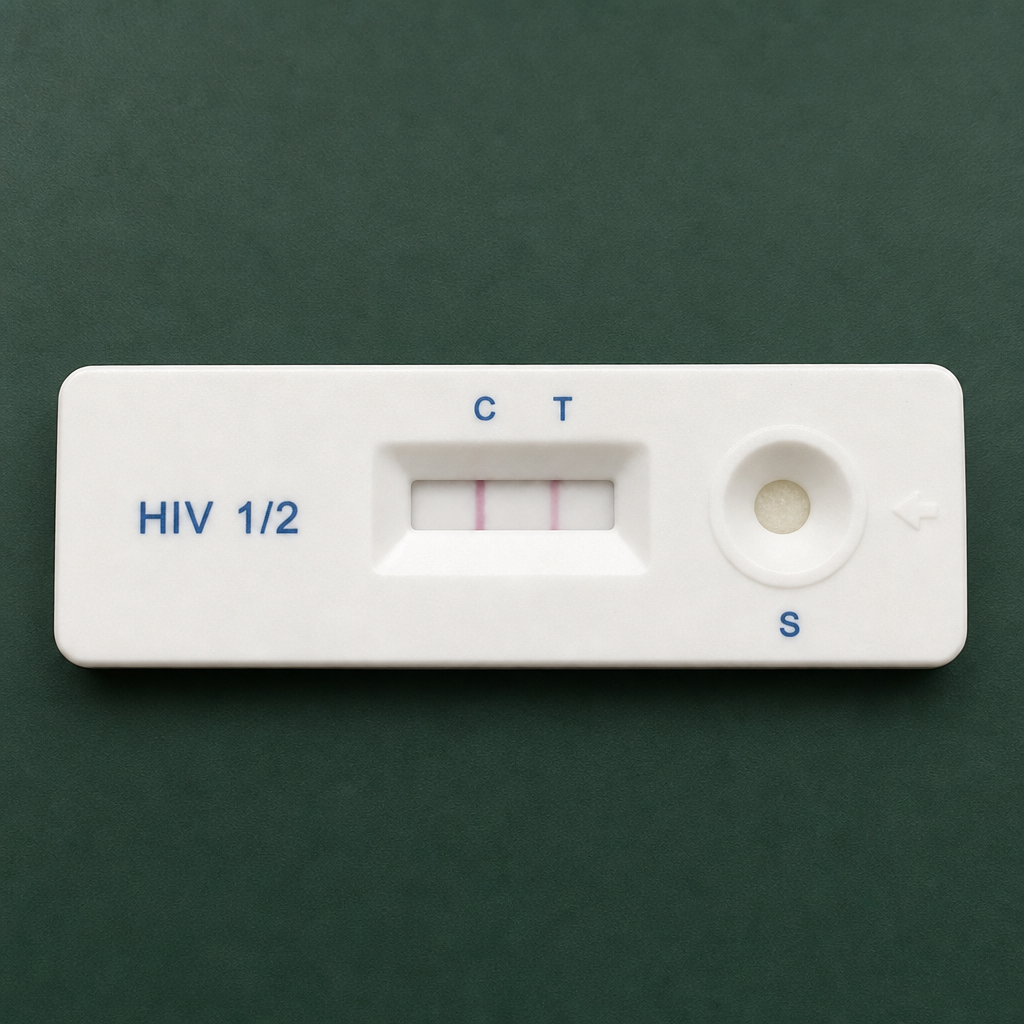
Which of the following is the principle of this test?
Which phospholipid is used to investigate syphilis by the reagin test?
A 31-year-old male patient complains of fatigue, oral candidiasis, and axillary lymphadenopathy. He reports engaging in high-risk behavior 6 years ago during a trip to eastern and southern Africa. His prior HIV test was reported as negative. Which one of the following diagnostic steps would be most appropriate?
What is the diagnostic test of choice for neurosyphilis?
MacConkey medium is an example of which type of culture medium?
A child presents with fever, sore throat, cough, and a membrane over the tonsils. A nasal swab is taken. On which culture medium would diagnosis be earliest?
Mycobacterium tuberculosis is differentiated from other atypical mycobacteria by which test?
A 55-year-old female patient presents with duodenal ulcer. What is the most sensitive test to detect Helicobacter pylori?
The Sereny test is positive for which of the following bacteria?
What is the best rapid diagnostic test for the etiology of acute pyogenic meningitis?
Practice by Chapter
Specimen Collection and Transport
Practice Questions
Microscopy in Microbiology
Practice Questions
Culture Methods and Media
Practice Questions
Bacterial Identification Techniques
Practice Questions
Antimicrobial Susceptibility Testing
Practice Questions
Serological Diagnosis
Practice Questions
Molecular Diagnostic Methods
Practice Questions
Rapid Diagnostic Tests
Practice Questions
Point-of-Care Testing
Practice Questions
Automation in Microbiology Laboratory
Practice Questions
Quality Control in Diagnostic Microbiology
Practice Questions
Interpretation of Microbiological Reports
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app