
Diagnostic Microbiology — MCQs

On this page
Which of the following is the enrichment medium for Vibrio cholera?
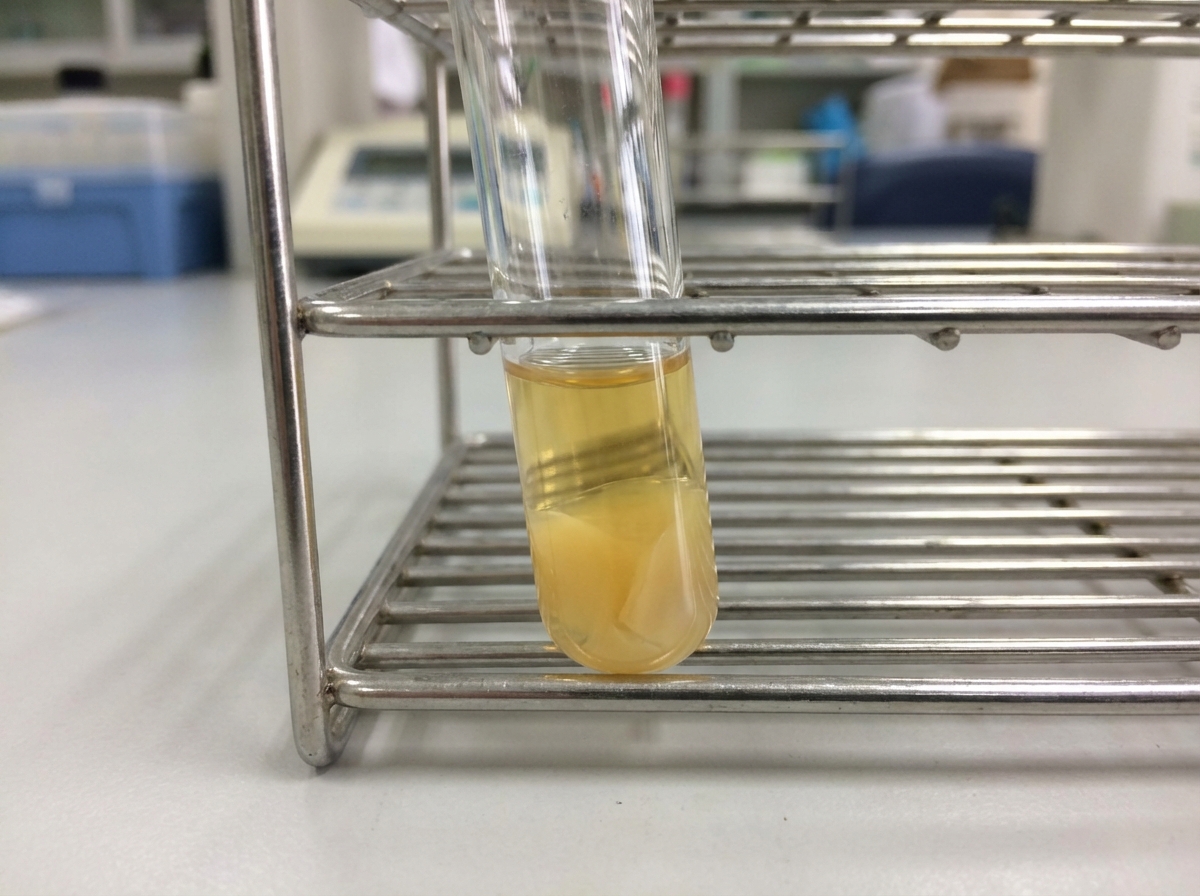
Which enzyme is responsible for this test?
Recent Hepatitis infection is best diagnosed by?
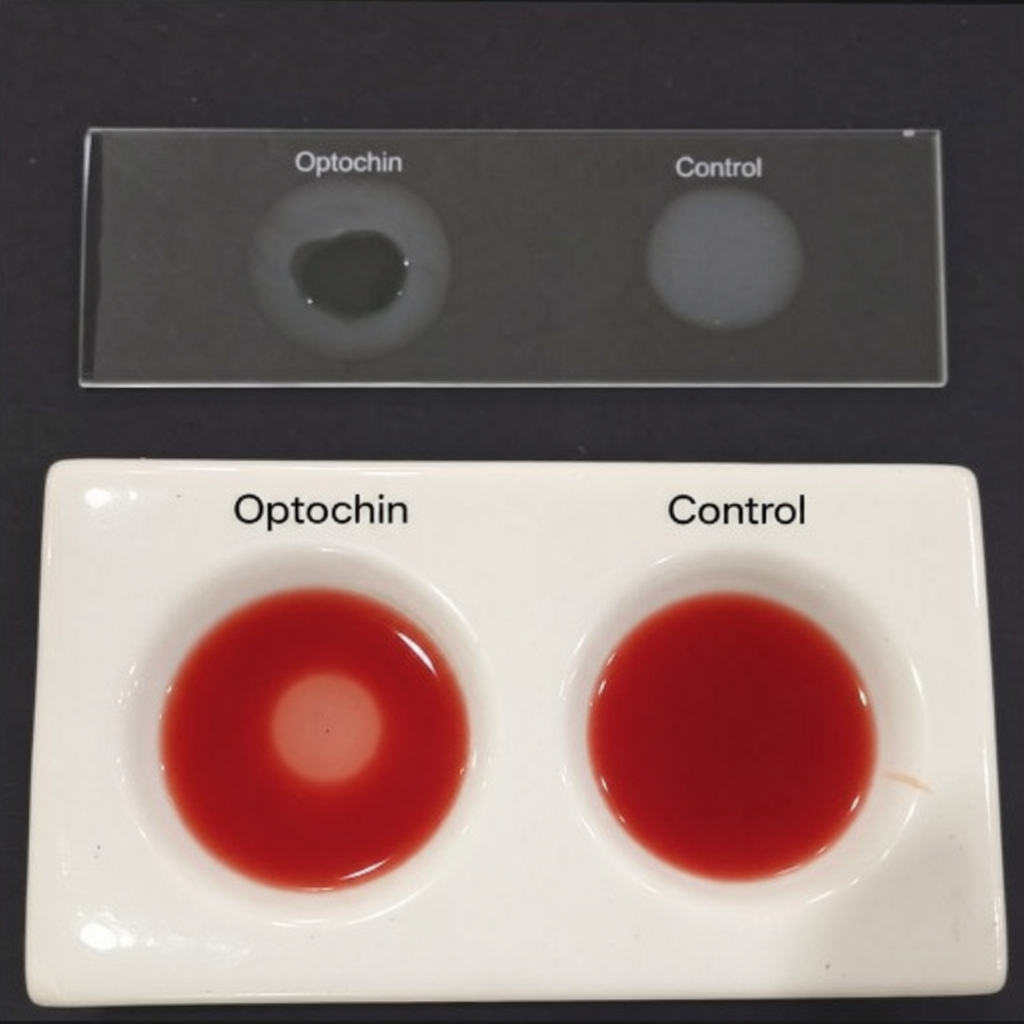
Which of the following organisms is identified by this test?
The Dienes phenomenon is used for the identification of which of the following?
All are tests used to assess the treatment response in Helicobacter pylori infection, EXCEPT:
Which of the following tests is best used in the diagnosis of congenital syphilis?
Radio-metric BACTEC detects the growth of M. tuberculosis in approximately how much time?
A 20-year-old male patient presents with a genital discharge described as resembling the flow of seeds. He reports a history of sexual intercourse with a commercial sex worker 5 days prior to presentation. What culture medium is typically used for the isolation of the causative organism?
What is the best serological test to diagnose the prodromal phase of Hepatitis A infection?
Practice by Chapter
Specimen Collection and Transport
Practice Questions
Microscopy in Microbiology
Practice Questions
Culture Methods and Media
Practice Questions
Bacterial Identification Techniques
Practice Questions
Antimicrobial Susceptibility Testing
Practice Questions
Serological Diagnosis
Practice Questions
Molecular Diagnostic Methods
Practice Questions
Rapid Diagnostic Tests
Practice Questions
Point-of-Care Testing
Practice Questions
Automation in Microbiology Laboratory
Practice Questions
Quality Control in Diagnostic Microbiology
Practice Questions
Interpretation of Microbiological Reports
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app