
Bacteriology — MCQs

On this page
A 12.6-month-old baby was brought with difficulty in feeding. The child was found to be hypotonic with a weak gag. The child is on breast milk, and the mother also gives honey to the child during periods of excessive crying. What is the causative agent?
Which biochemical test differentiates Corynebacterium diphtheriae from Corynebacterium pseudotuberculosis?
Genital ulcers are seen in all except:
Which of the following statements regarding diphtheria is true?
All of the following are indications for CSF examination in adults with all stages of Syphilis, except?
Which bacterial toxin's mechanism of action does not involve an increase in intracellular cyclic AMP (cAMP)?
Which of the following conditions is not caused by beta-hemolytic Streptococcus pyogenes?
Which of the following statements about non-typhoidal Salmonella is NOT true?
A child developed symptoms of food poisoning 4 hours after ingesting fried rice, with Bacillus cereus suspected. Which of the following is TRUE about the symptoms of Bacillus cereus food poisoning in this case?
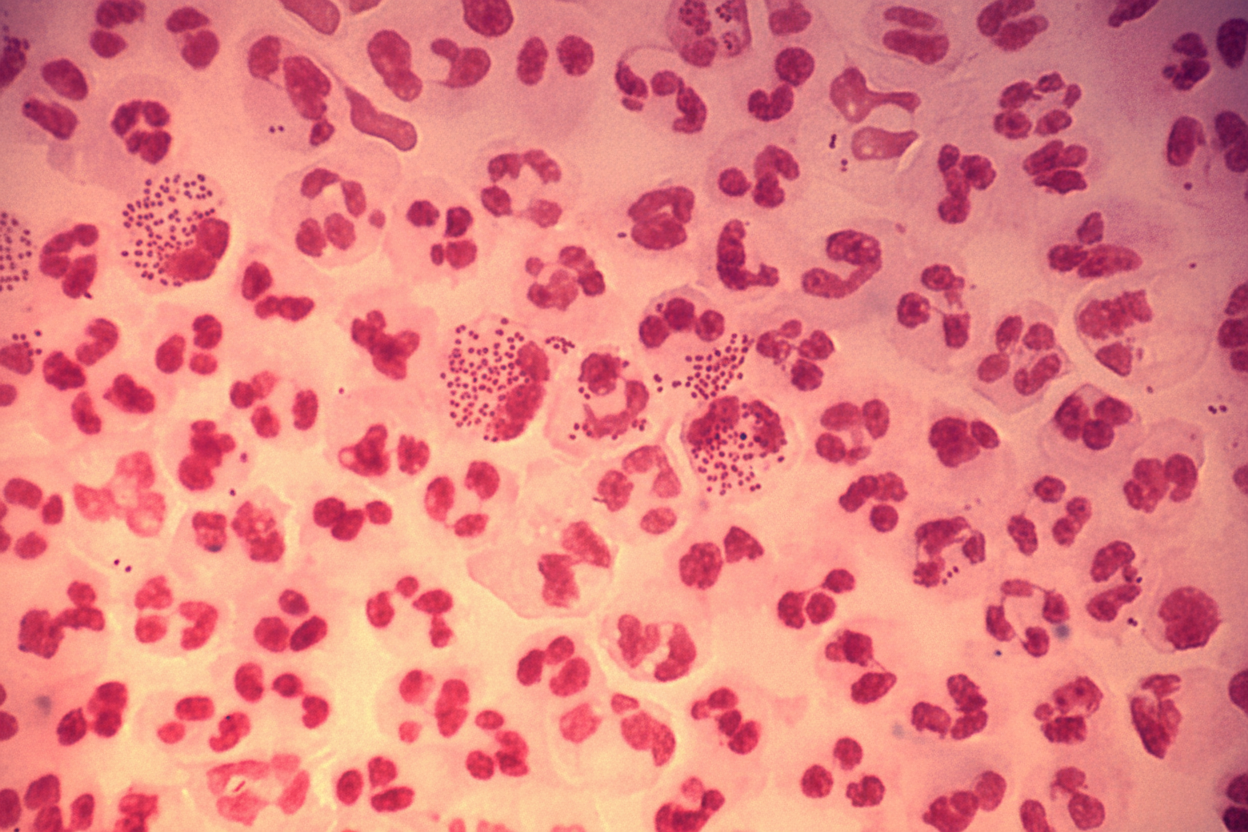
A 35-year-old male presents with a history of urethral discharge for the last three days. A Gram stain smear of the discharge is shown. Which of the following is true regarding the likely etiology?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app