
Bacteriology — MCQs

On this page
Electron microscopic examination of the bacterial flora of necrotising ulcerative gingivitis indicates the presence of microorganisms within non-necrotic tissues in advance of other bacteria. What are the organisms involved?
Which of the following is true regarding the 8th pandemic of cholera?
Haemophilus influenzae has been isolated from the CSF of a two-year-old boy suffering from meningitis. The strain is beta-lactamase producing and resistant to chloramphenicol. What is the most appropriate antimicrobial in this situation?
Which in vitro test is used to determine the virulence of pneumococcus?
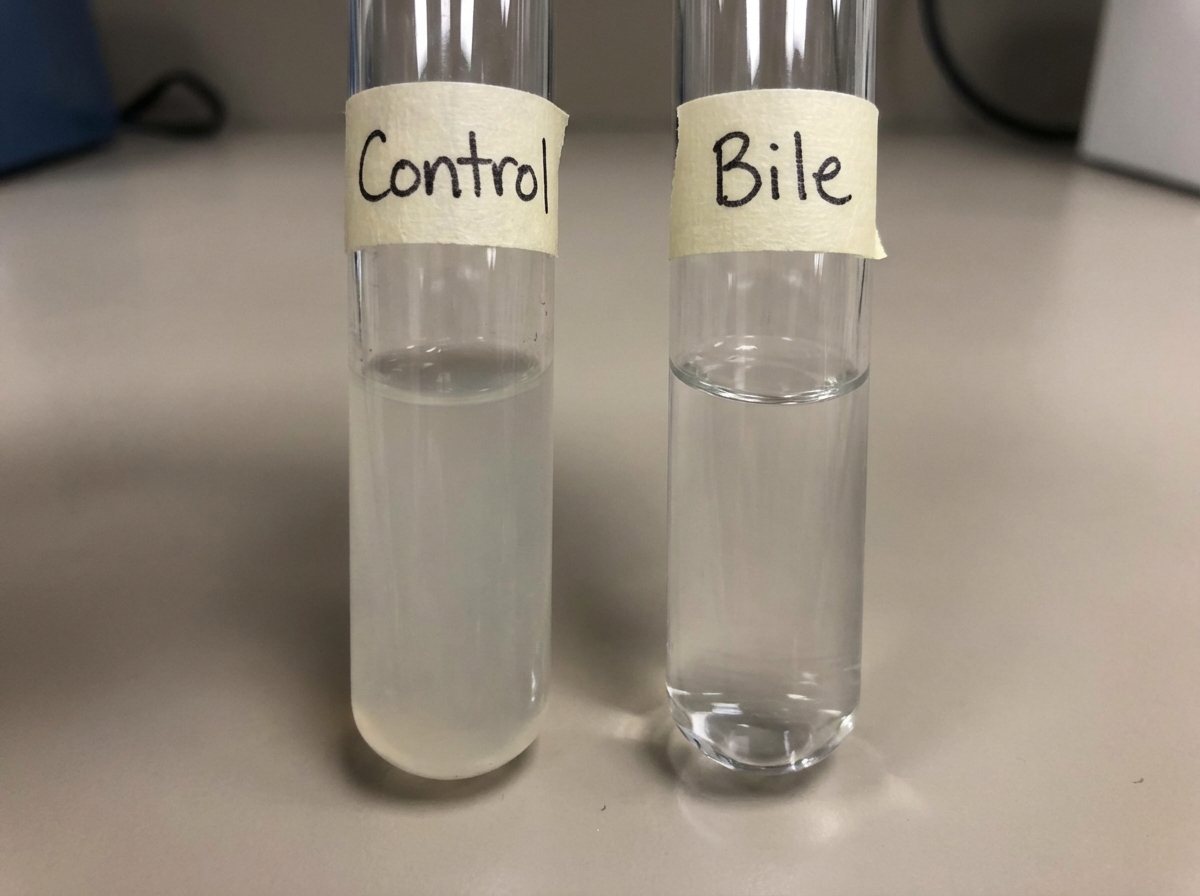
Which organism gives the demonstrated positive bile-solubility result shown in the illustration?
Which of the following is NOT true about Helicobacter pylori?
Chlamydial infection is associated with which of the following?
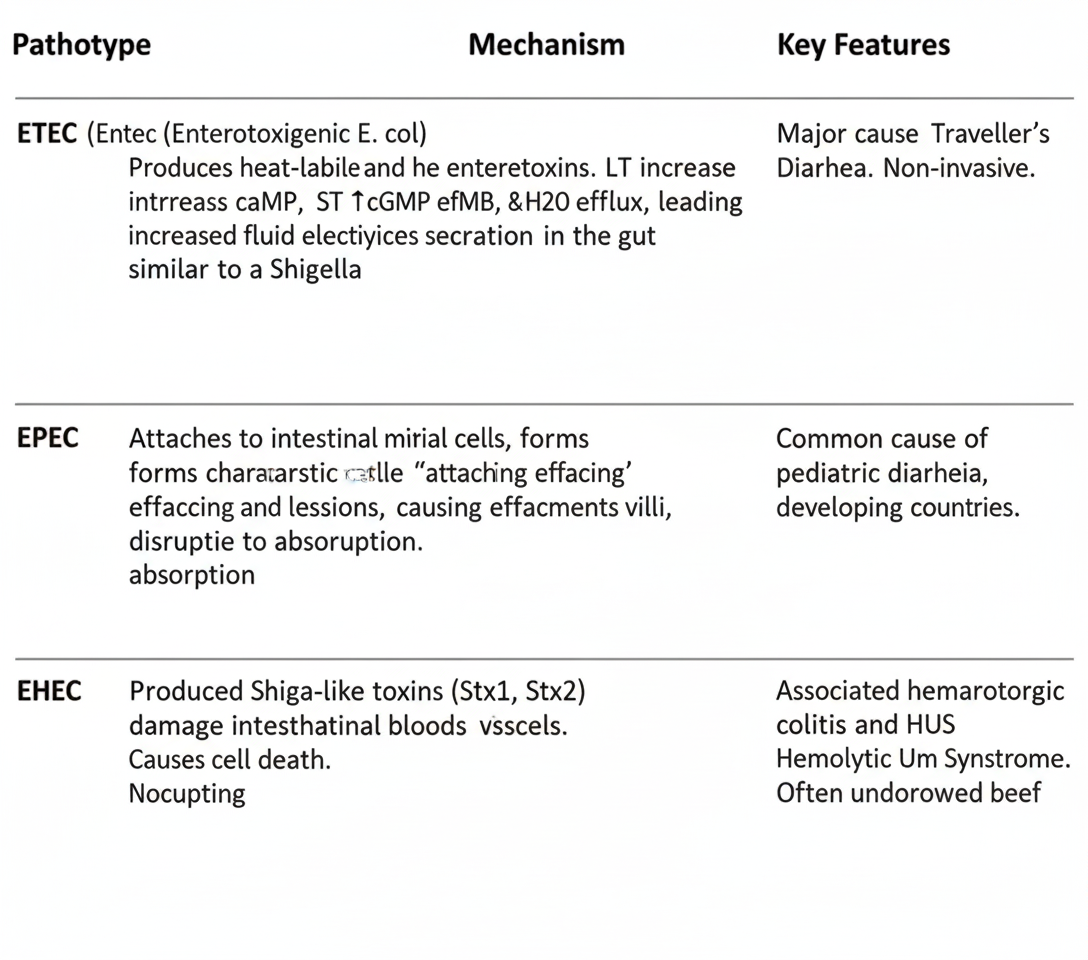
A 6-month-old infant in a developing country presents with profuse watery diarrhea and dehydration. Stool cultures grow E. coli. Electron microscopy of intestinal biopsy shows destruction of microvilli with intimate bacterial attachment to the epithelial surface, forming characteristic pedestal structures. Which E. coli pathotype is responsible?
Which one of the following organisms is the most frequent cause of acute pyogenic meningitis in adults?
Which anaerobic bacterium is commonly found in the cervix or vagina, maintains a low pH, and protects against other bacterial infections?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app