
Bacteriology — MCQs

On this page
A 68-year-old male patient with 3rd-degree burn wounds affecting 25% TBSA was admitted to the hospital and treated with intravenous fluids and analgesics. After 8 days of hospital admission, the patient develops fever and leukocytosis. On examination, there is erythema and swelling around the wound. Exudate from this wound is positive for gram-negative, oxidase-positive bacilli which do not ferment sugars. What is the drug of choice for this infection?
Absence of Vi-antibody in a typhoid patient indicates what regarding prognosis?
A boy presented with multiple non-suppurative osteomyelitic dactylitis with sickle cell anaemia. What is the likely causative organism?
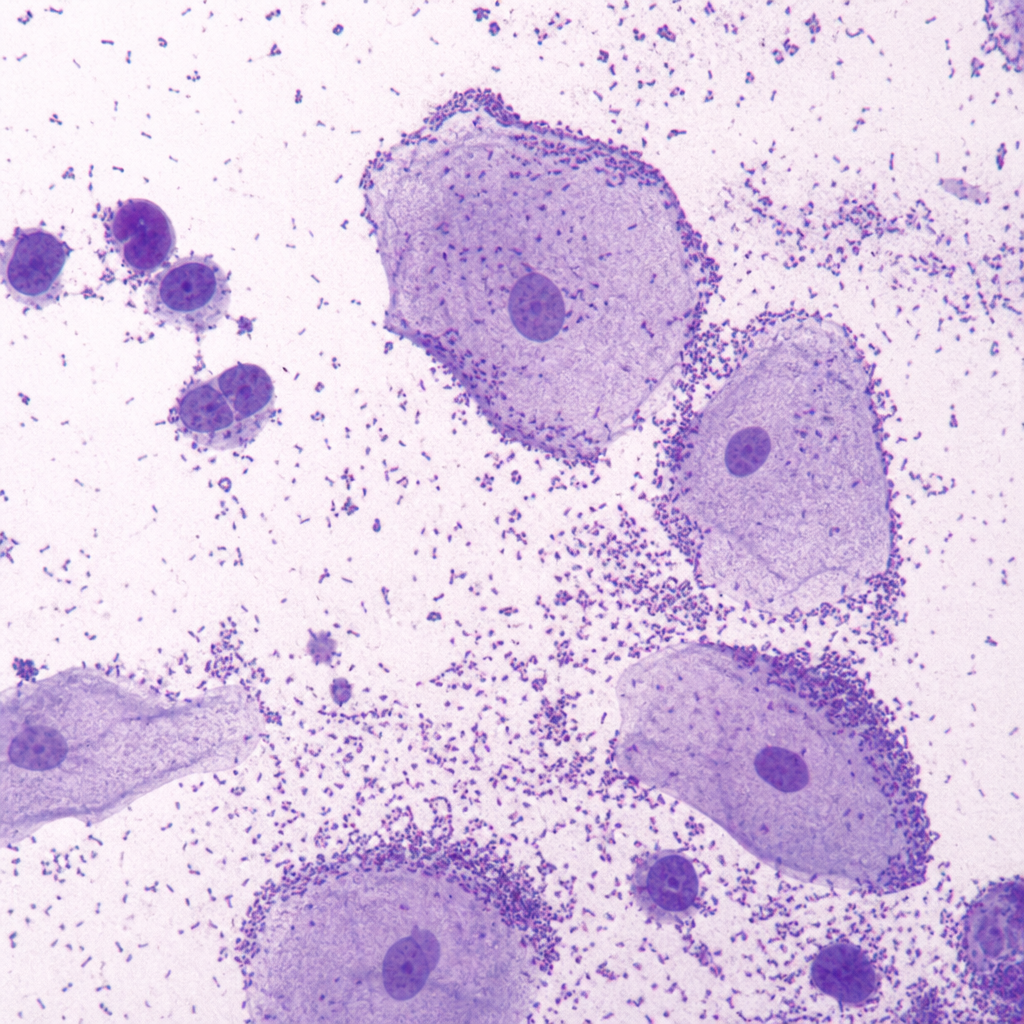
A 40-year-old woman presented with complaints of profuse vaginal discharge. There was no discharge from the cervix on speculum examination. The microscopy image of the vaginal discharge is shown above. Which of the following is NOT a microscopic finding expected in bacterial vaginosis?
What is the most common cause of clostridial food poisoning?
What is a characteristic of H. Pylori?
Which of the following statements regarding H. pylori is false?
Painless diarrhea occurs with which of the following pathogens?
Which of the following statements regarding gullwing-shaped bacteria is FALSE?
Staphylococcus aureus produces a superantigen that contributes to massive cytokine release and polyclonal T-cell activation. Which of the following best fits this description of a superantigen?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app