
Bacteriology — MCQs

On this page
A patient presents with fever for 3 weeks. On examination, splenomegaly is observed. Ultrasonography reveals a hypoechoic shadow in the spleen near the hilum. Gram-negative bacilli are isolated on blood culture. Which of the following is the most likely causative organism?
Which of the following statements about tetanus is FALSE?
A seven-year-old boy presented with high-grade fever, headache, disorientation, and projectile vomiting. Examination revealed neck rigidity and a positive Kernig's sign. Lumbar puncture was performed. Gram staining of the cerebrospinal fluid (CSF) showed Gram-negative cocci. What is the most likely cause of this infection?
A 40-year-old man presents with a nonproductive cough, malaise, sinusitis, and sore throat. His chest x-ray reveals patchy infiltrates in the upper right lung without consolidation. He denies recent exposure to new pets. Sputum Gram-stain shows poorly staining Gram-negative rods. Laboratory cultures on standard media are unsuccessful, but the organism grows in tissue culture. What bacterium is most likely causing this infection?
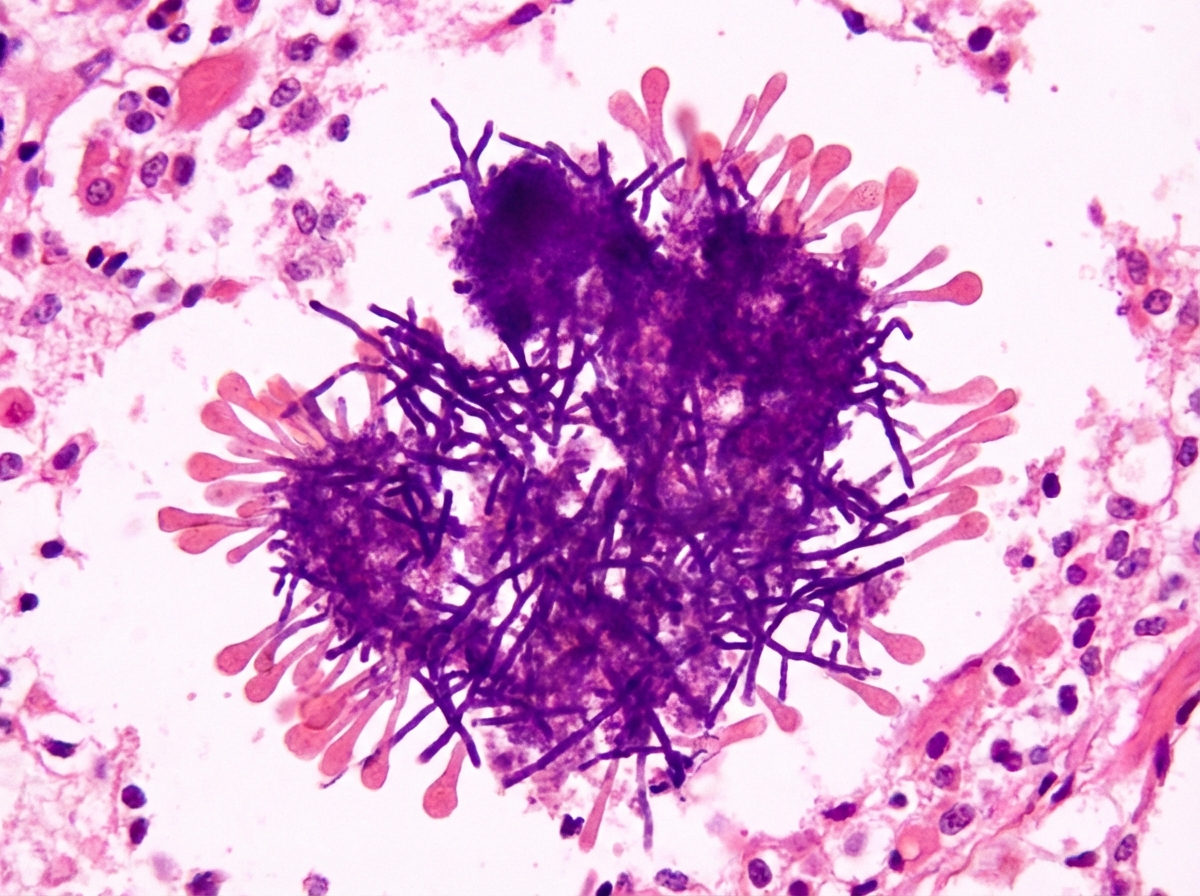
A 50-year-old female patient presented with a painless, exudative swelling of the right jaw, following trauma to the same area. Pus sent for culture revealed a sulfur granule on macroscopic examination. A histologic section of the exudate is provided. What is the drug of choice for this condition?
What is the most common organism causing food poisoning from canned food?
What is the most common causative organism of septic arthritis in a 2-year-old child?
What is the most common infection caused by Streptococcus pneumoniae?
All of the following statements regarding Chlamydia are true, except?
Which of the following is NOT true regarding pseudomembranous colitis?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app