
Bacteriology — MCQs

On this page
Which of the following statements regarding Salmonella infection is true?
Bannwah's syndrome develops secondary to infection with which of the following organisms?
Actinomycosis is sensitive to which of the following antibiotics?
What is the ideal percentage of CO2 required for the growth of Brucella abortus?
Which mycobacterium exclusively affects the skin?
Which of the following bacteria is NOT motile?
What type of diarrhea is caused by Vibrio cholerae?
What is the most common microorganism found in pediatric subacute infective endocarditis?
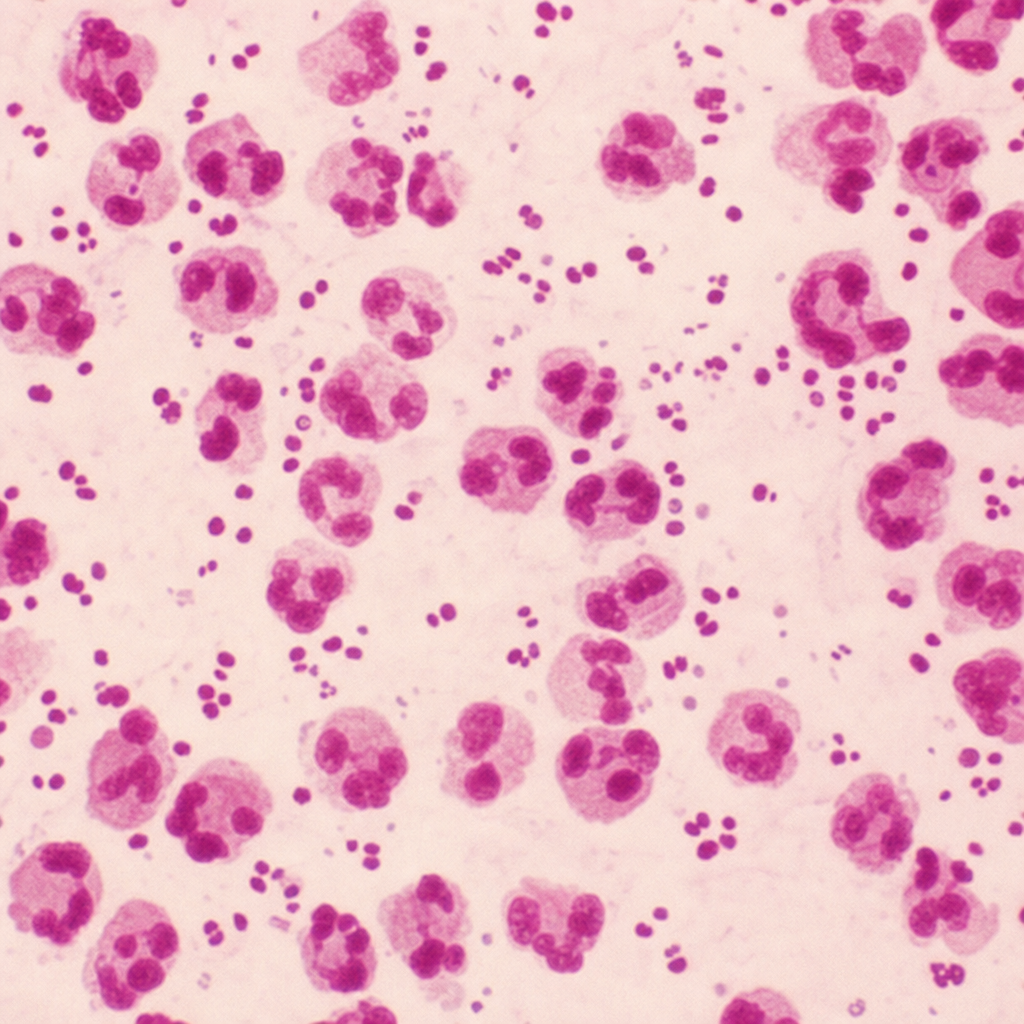
A 25-year-old sexually active unmarried male presents with urethral discharge after unprotected sex with a sexual worker. A Gram stain was provided; what is the most likely causative organism?
Which of the following statements about Corynebacterium diphtheriae is incorrect?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app