
Bacteriology — MCQs

On this page
Myocardial abscess is most common in acute endocarditis caused by which organism?
Which of the following is a tap water scotochromogen?
A 3-year-old child with cystic fibrosis presents with weight loss, irritability, and a chronic productive cough. On physical exam, he is febrile and lung exam reveals intercostal retractions, wheezing, rhonchi, and rales. Chest x-ray demonstrates patchy infiltrates and atelectasis. Gram's stain of the sputum reveals slightly curved, motile gram-negative rods that grow aerobically. Which of the following diseases is most commonly caused by the microorganism responsible for this child's pneumonia?
Which of the following statements about Botulism is false?
Which of the following statements is true regarding Streptococcus pneumoniae?
Which organism commonly causes an 'appendicitis-like syndrome'?
Mycoplasmas differ from chlamydiae in that they are
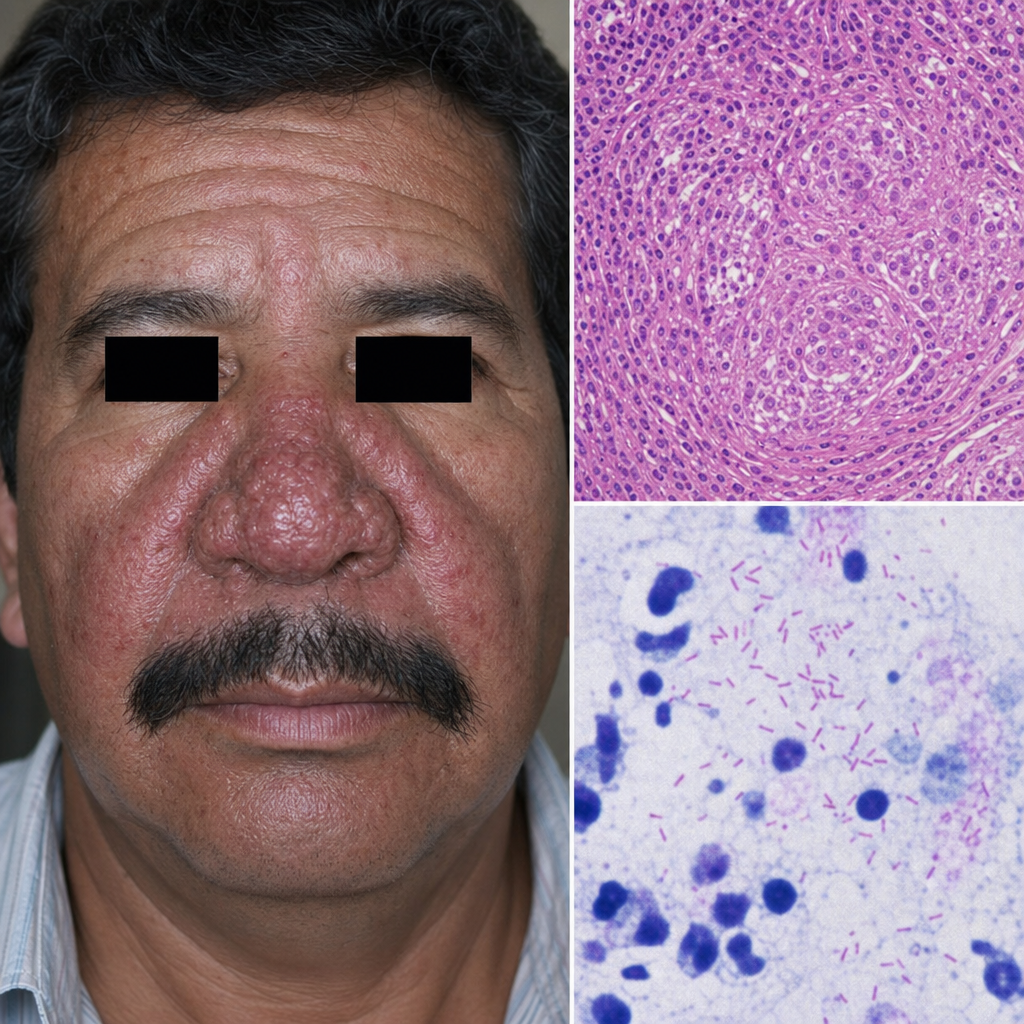
A man from Mexico presents with a clinical finding that, upon biopsy, reveals the presence of gram-negative bacilli. What is the most likely causative agent?
A 70-year-old nursing home patient refused the influenza vaccine and subsequently developed influenza. She died of acute pneumonia 1 week after contracting the "flu." What is the most common cause of acute post-influenzal pneumonia?
A man presented with diarrhea three days after consuming uncooked meat. Stool examination revealed comma-shaped organisms with red blood cells and white blood cells. What is the causative organism?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app