
Bacteriology — MCQs

On this page
Bacterial endocarditis is most commonly caused by which organism?
True about the HACEK group of bacteria?
Which of the following Corynebacterium species produces a toxin similar to that of diphtheria toxin?
All of the following are true about Listeria except?
What is true about Staphylococcus aureus?
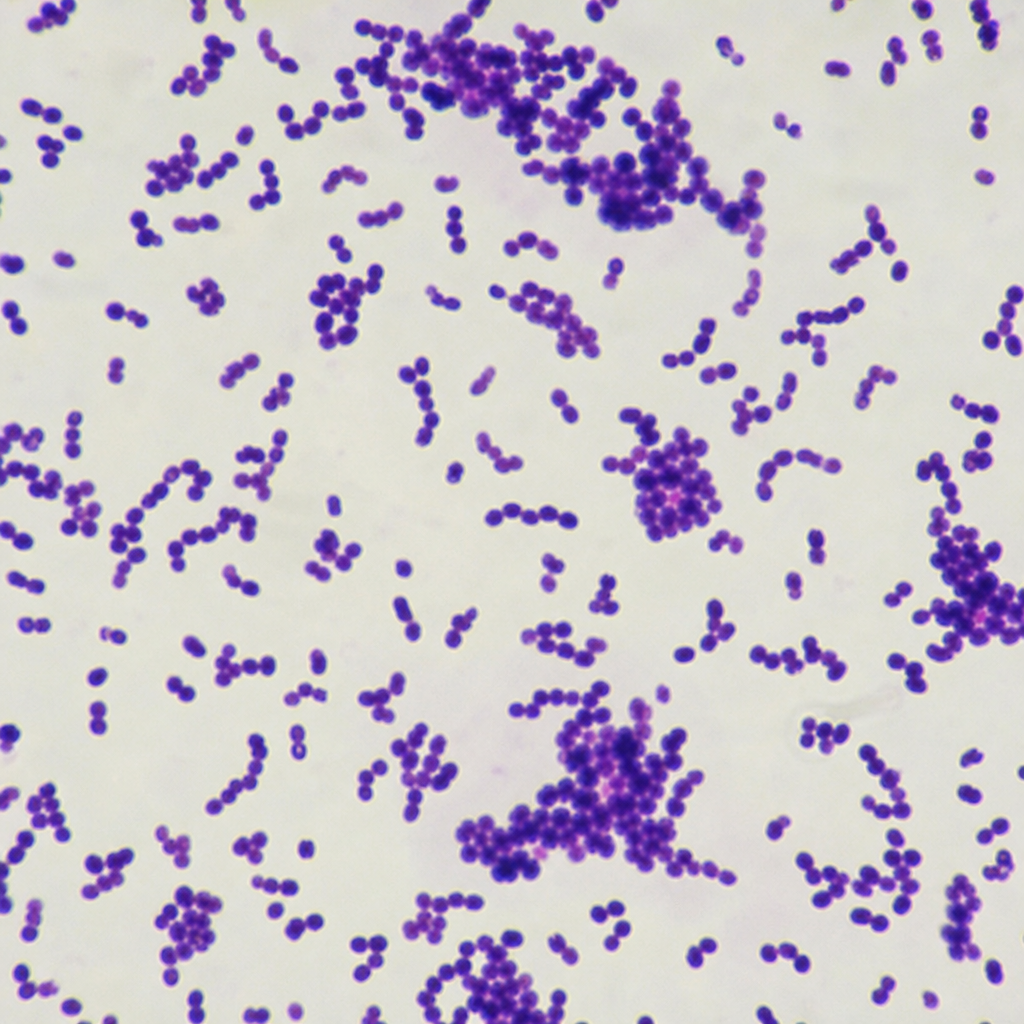
A 34-year-old pregnant female presented to the ER with fever, backache, headache, and myalgias. Blood cultures were collected and subjected to examination. Microbiological examination revealed positive motility at 25 degrees Celsius, catalase positivity, esculin positivity, and positive growth in 6.5% NaCl. Gram staining revealed the following characteristics of the organism isolated. Which of the following is the most common route of transmission of this organism?
A 65-year-old diabetic man presents with a severe productive cough producing thick, bloody sputum with a "currant-jelly" appearance. MacConkey agar reveals pink colonies, and routine laboratory media shows large mucoid colonies. Which of the following organisms is most likely responsible for this patient's pneumonia?
Which of the following does not cause invasive diarrhea?
Phage typing is widely used for the intraspecies classification of which of the following bacteria?
What is the most common organism causing osteomyelitis?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app