
Bacteriology — MCQs

On this page
A six-month-old male child presented with fever, inability to feed, and seizures. On examination, the child had altered sensorium and neck rigidity. Cerebrospinal fluid (CSF) analysis suggested pyogenic meningitis. Microscopic examination revealed Gram-negative coccobacilli, and culture on blood agar showed a specific phenomenon. What is this phenomenon?
A patient presents to the emergency department with a history of persistent fever and cough. Radiological features are suggestive of pneumonia. Sputum examination cultures reveal aerobic branching Gram-positive filaments that are partially acid-fast. Which of the following is the most likely etiological agent?
Which condition shows organisms with a characteristic "school of fish" appearance in stained smears?
Soft chancre is a feature of which of the following?
Mycoplasma pneumoniae is an infectious agent that:
Which of the following pleomorphic coccobacilli shows the satellite phenomenon on blood agar?
A 55-year-old man presents with low-grade fever, cough, and increased sputum production for 5 days. He has a history of chronic bronchitis and diabetes. Which of the following structures is NOT used by the causative organism to cause the disease?
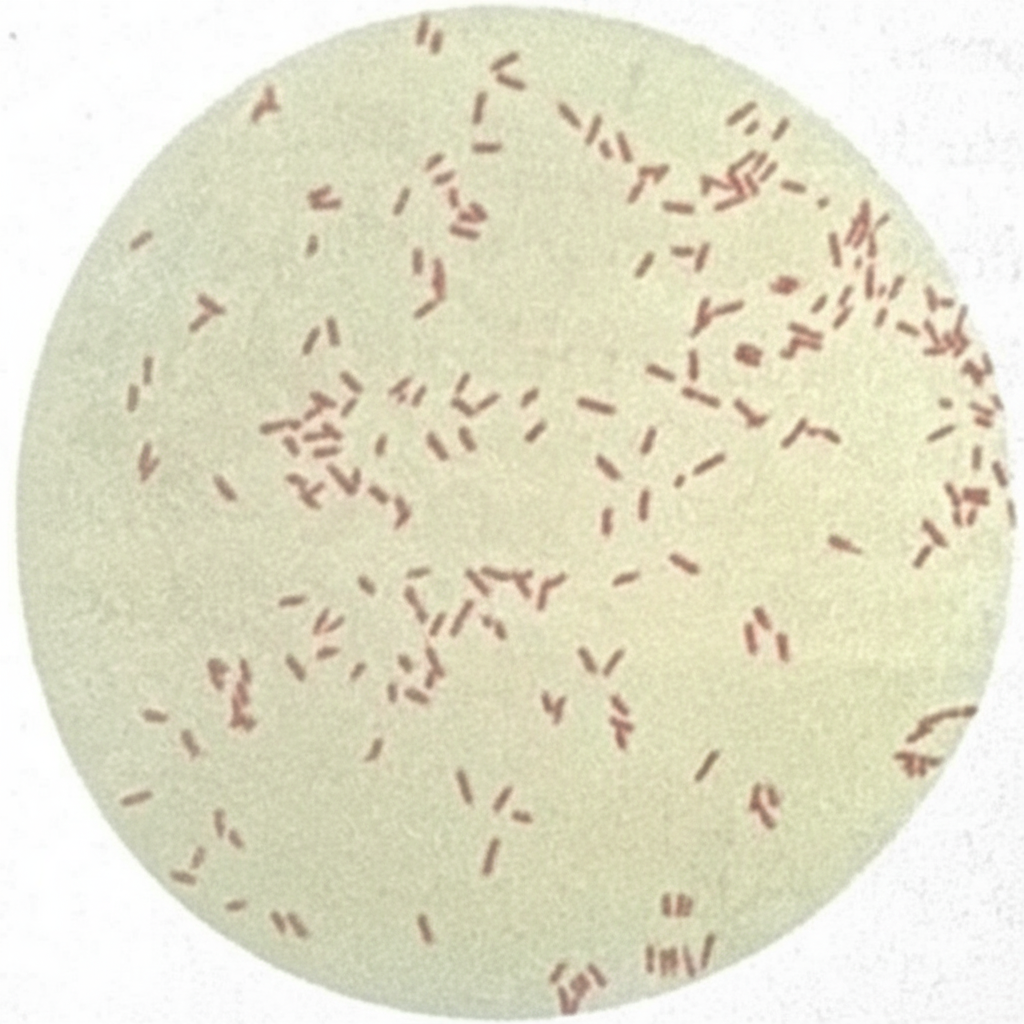
Which category of organism is shown on this Gram stain?
What is the most common organism causing meningitis in patients with a cerebrospinal fluid (CSF) leak?
Streptococcus agalactiae belongs to which Lancefield group?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app