
Bacteriology — MCQs

On this page
A 10-month-old child presents with a two-week history of fever, vomiting, and alteration of sensorium. A cranial CT scan reveals basal exudates and hydrocephalus. What is the most likely etiological agent?
Which of the following statements about Staphylococcus epidermidis is true?
Which of the following statements about the lepromin test is true?
Endotoxins have all but one of the following properties?
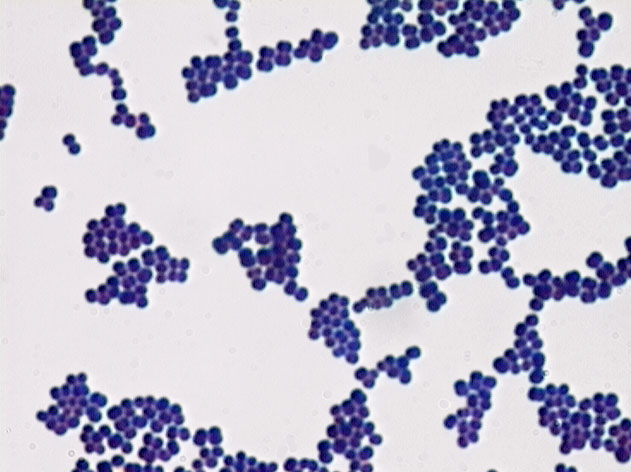
The following gram stain image shows which bacteria? The organism is also found to be coagulase-positive.
Which organism causes toxic shock syndrome?
Vector of trench fever is which one of the following?
Which of the following statements about Streptococcus is false?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app