
Bacteriology — MCQs

On this page
A 40-year-old patient with a history of intravenous drug use presents with fever and a new heart murmur. Blood cultures grow gram-positive cocci in chains. What is the most likely organism?
Which microorganism is most likely to cause a rapidly progressive, painful infection with gas formation in the tissues?
A marine biologist working with aquatic samples presents with skin lesions and lymphadenopathy. Culture of the lesion yields a water-adapted organism. What is the most likely pathogen and its natural habitat?
A patient with chronic sinusitis has nasal discharge that is positive for gram-positive, coagulase-positive cocci. What is the most likely causative organism?
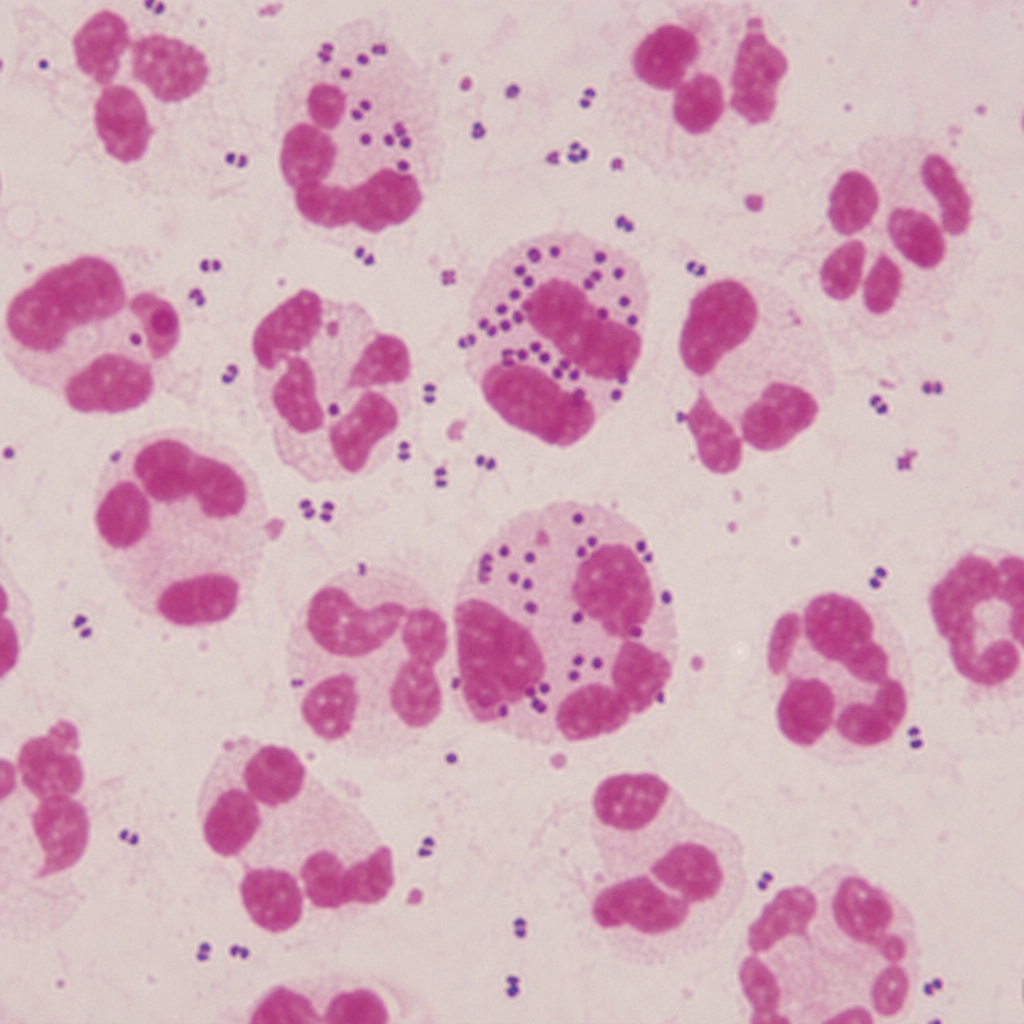
What is the MOST COMMON causative organism for the condition depicted in the provided image?

A Gram stain of cerebrospinal fluid from a patient with acute bacterial meningitis is shown in the image. Identify the following bacterium from the image.
Burkholderia cepacia is resistant to which of the following antibiotics?
What is the most common cause of acute salpingitis?
What is the cause of Ritter disease?
Which of the following diseases is caused by Borrelia?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app