
Bacteriology — MCQs

On this page
What is the clinical significance of the coagulase enzyme produced by Staphylococcus aureus?
Which organism is the most common cause of neonatal urinary tract infections?
A 55-year-old male with diabetic neuropathy presents with a rapidly progressing necrotic lesion on his foot. Which organism is most likely responsible?
A 22-year-old woman presents with dysuria, frequency, and urgency. A urine culture reveals a lactose-fermenting Gram-negative rod. What is the most likely causative agent?
A 29-year-old male reports a red, painful lump on his back that has ruptured and drained pus. Which organism is the most likely cause?
A 12-year-old girl presents with fever, shortness of breath, and cough. A chest X-ray reveals complete consolidation of the left lower lung lobe. What is the most probable organism?
A 2-year-old child presents with fever and a maculopapular rash. Blood culture grows gram-positive cocci in chains that are catalase-negative. Which organism is likely responsible?
Which disease is characterized by severe watery diarrhea and is associated with a toxin-producing bacterium?
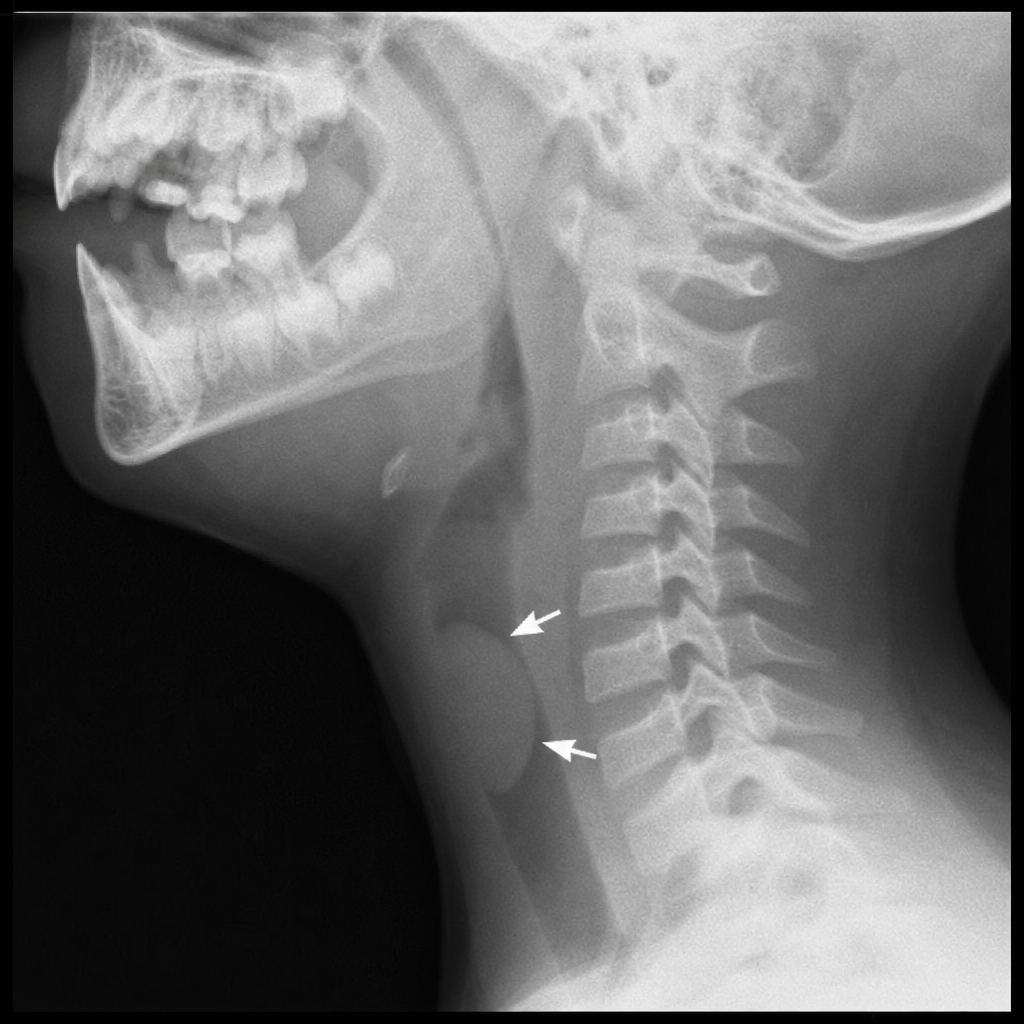
An unvaccinated child presents with a sudden onset of drooling, dysphagia, and respiratory distress. A lateral neck X-ray reveals a thumbprint sign. What is the most likely cause?
A 60-year-old patient develops a central line infection with gram-positive cocci that are catalase-positive and coagulase-negative. What is the most likely pathogen?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app