
Bacteriology — MCQs

On this page
Which of the following doesn't cause urethritis in males?
True about lepra bacilli is
Which of the following is the aetiological agent most often associated with Epiglottitis in children -
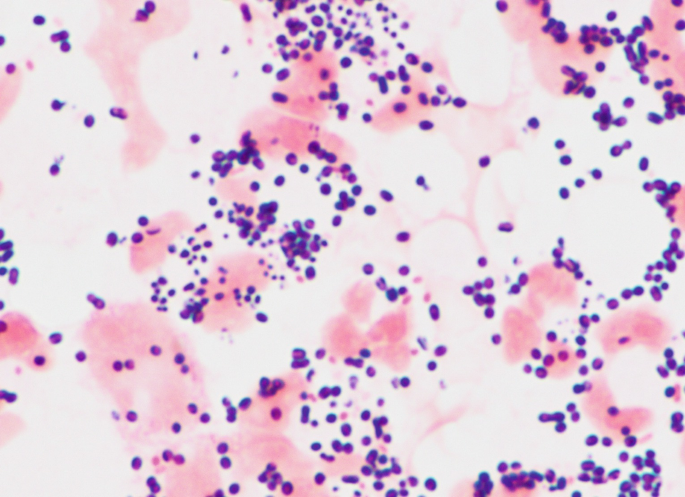
A 9 years old child presented to OPD with complaints of high grade fever, vomiting, one episode of seizure. CSF examination was done and Gram staining of the culture showed the following finding. What is the probable causative agent?
A 12 year old boy presents with vomiting within 3 hours of consumption of food at a party. What is the likely causative organism responsible for the symptoms?
A 29 year old male was brought to ED with complaints of nausea, vomiting and abdominal cramps 3-4 hours after eating meat at dinner. What is the likely cause of this condition?
Superantigen is produced by which of the following?
Urethritis in males is not caused by:
Gram stain of CSF shows gram-negative diplococci. Culture grows on Thayer-Martin medium. Most likely organism?
Which microorganism causes pseudomembranous colitis?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app