
Bacteriology — MCQs

On this page
Following acute pharyngitis, a patient was on broad spectrum antibiotics. One week later he developed watery diarrhoea with a foul odour and abdominal cramps. Antibiotic induced colitis is confirmed. What is the most common cause of antibiotic induced colitis?
Ludwig angina is usually caused by
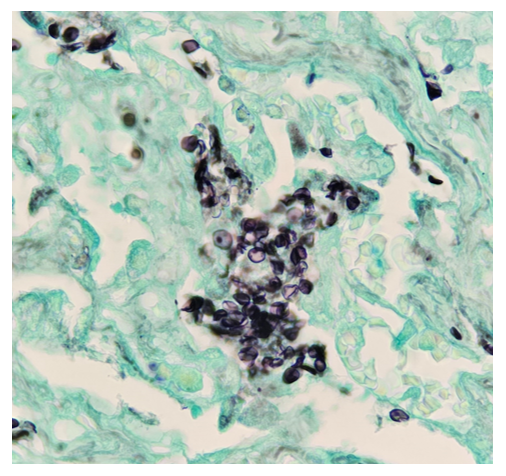
A 44-year-old female presented to OPD with complaints of pallor, fatigue, weakness, palpitations and dyspnea on exeion. Blood tests were conducted, which revealed, Anemia Thrombocytopenia Leukocytosis with neutropenia and increased blasts in the peripheral blood smear. Peripheral blood smear The patient was diagnosed with leukemia and she underwent allogenic stem cell transplantation for the same. After 24 days, she again presented with hypotension, tachycardia, and spO2 of 88% along with a new rash from which biopsy was taken and GMS (Grocott's Methenamine Silver) staining was done. Lab findings revealed severe Neutropenia. Which is the most likely organism causing the above skin condition: -
Which one of the following gram-positive organisms is the most common cause of UTI among sexually active women?
All of the following statements about Botulism are true except:
In cystic fibrosis, the most common organism which causes early infection is
Phagosome-lysosome fusion in TB-infected macrophages is inhibited by -
Which of the following microorganisms causes Buruli ulcer?
CSF in meningococcal meningitis shows -
Most common organism causing UTI:
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app