
Bacteriology — MCQs

On this page
A patient presents with a history of pastry intake causing food poisoning. What is the most likely causative agent?
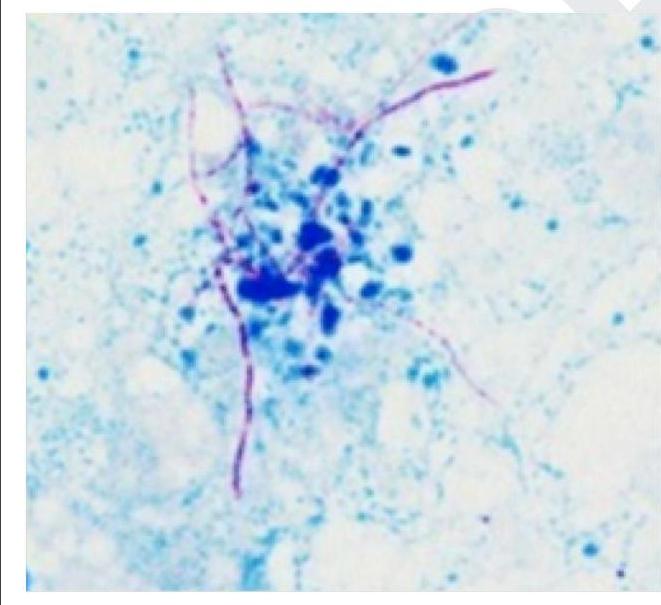
Which of the following is a gram-positive organism that shows the following appearance on Ziehl-Neelsen staining?
Which of the following microorganisms will be resistant to meropenem and aminoglycosides but sensitive to piperacillin tazobactam and cotrimoxazole?
A peculiar organism has resistance to azithromycin, but is sensitive to ticarcillin, clavulanic acid, cotrimoxazole. Identify the organism?
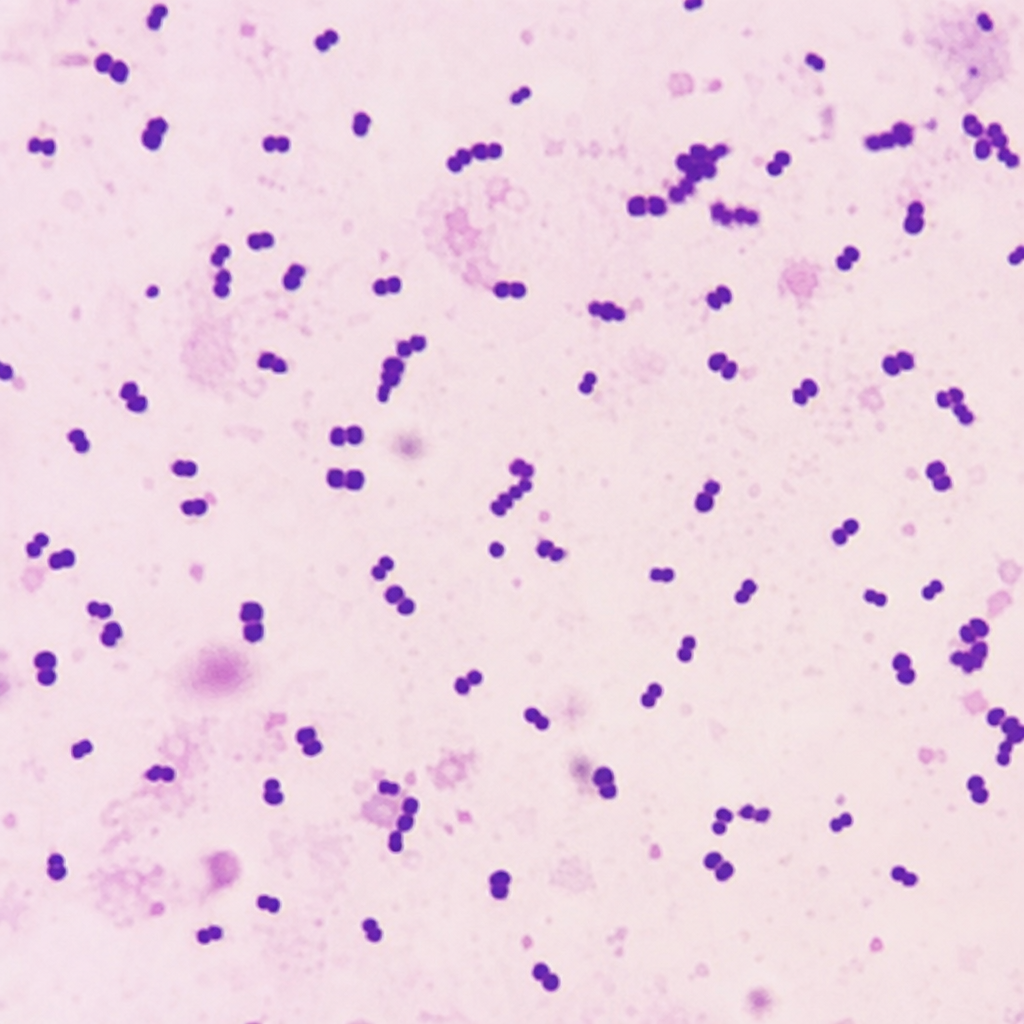
An elderly male presented with meningitis. The CSF sample was subjected to Gram staining, and the microscopy image is shown. Which of the following is a characteristic of the likely organism?
Which pathogen causes attachment - effacement lesion in the intestinal mucosa as shown in the image?

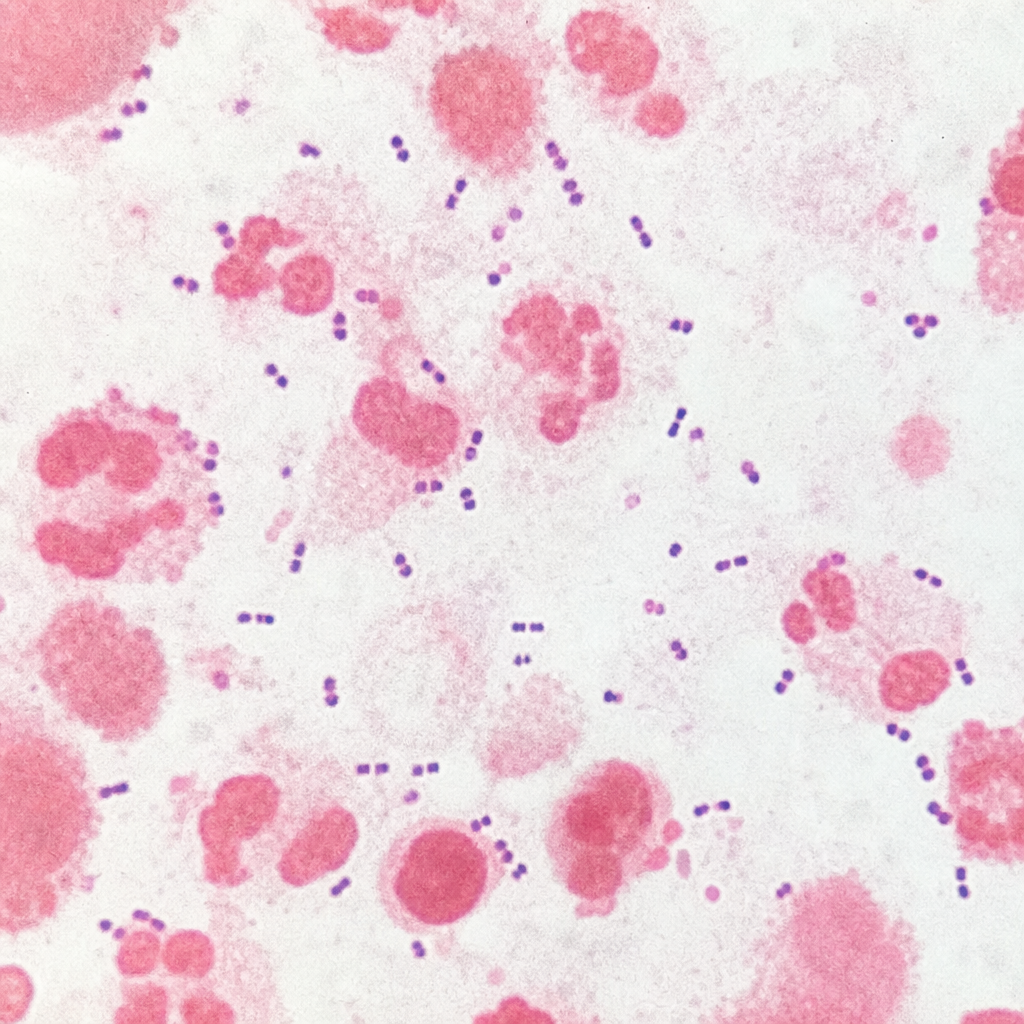
A patient presented with meningitis, and the CSF sample was subjected to gram staining and microscopy and appears as shown in the microscopic image given below. Which of the following features / tests will be characteristic of the organism?
A patient presented with meningitis, and the CSF sample shows Gram-negative diplococci on Gram staining and microscopy. Which of the following features/tests will be characteristic of the organism?
A 28-year-old man presents with painful inguinal lymphadenopathy and penile ulcers. The ulcers are painful, soft, and have undermined edges with purulent base. Gram stain shows small, pleomorphic gram-negative rods. Which virulence factor is responsible for the tissue destruction in this infection?
What is the mechanism by which Chlamydia trachomatis causes cellular damage in urethritis?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app