
Bacteriology — MCQs

On this page
A patient presents with sinus tracts on the foot, and a smear reveals filamentous organisms.
A 27-year-old patient presents with motheaten alopecia, moist perianal lesions, and an asymptomatic macular rash. What is the most likely causative organism?
A clinical specimen is examined under light microscopy and reveals small rod-shaped organisms arranged in clusters. What is the most appropriate description of these organisms?

A farmer presents with a subcutaneous wound on his foot with discharge. Microscopy of a white granule from the wound shows Gram-positive filamentous rods. What is the most likely organism?
A patient was diagnosed with Escherichia coli O157:H7 infection. In this designation, what does the "H" stand for?
A patient was admitted with bloody diarrhea after consumption of oysters. The organism exhibits the Kanagawa phenomenon. What is the correct organism?
An adult patient with a military background is admitted with a rash, fever, altered sensorium, and a deficiency of the membrane attack complex. What is the most likely etiological agent?
A male patient presents with white discharge from the urethra, as shown in the image. What is the most probable causative organism?
A group of people ate patty late at night and experienced bouts of vomiting early in the morning. What is the most likely cause?
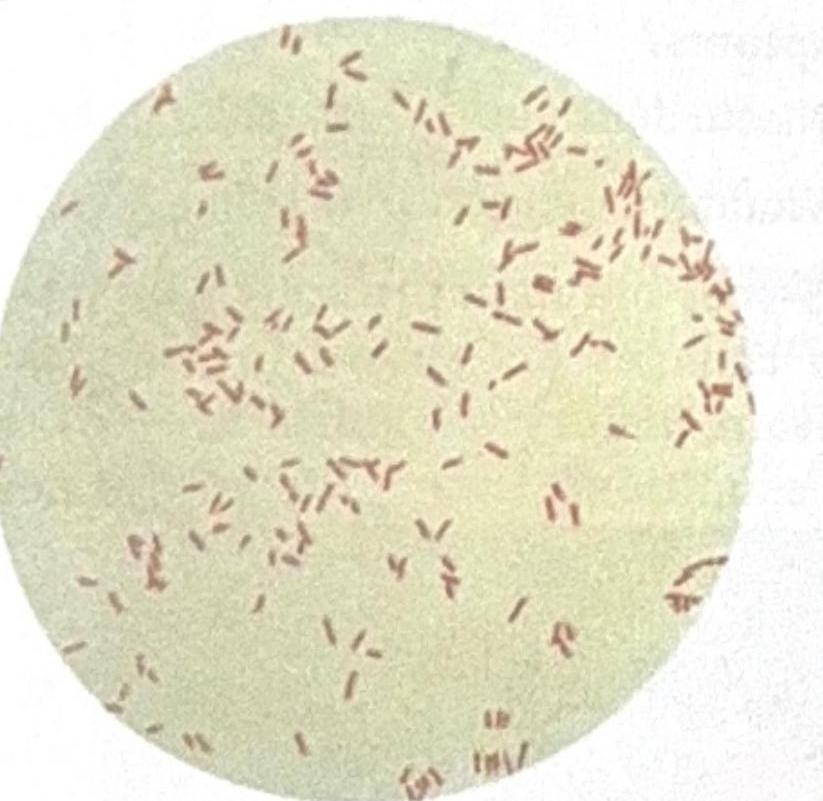
A patient presented with 70% burns, and a sample was collected from the burn site. The image shows Gram-negative rods, and the suspected organism is an obligate aerobe. What is the most likely causative microbe?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app