
Bacteriology — MCQs

On this page
All of the following toxins are produced by the organisms shown below except:
Identify the organism shown below. (AIIMS May 2017)
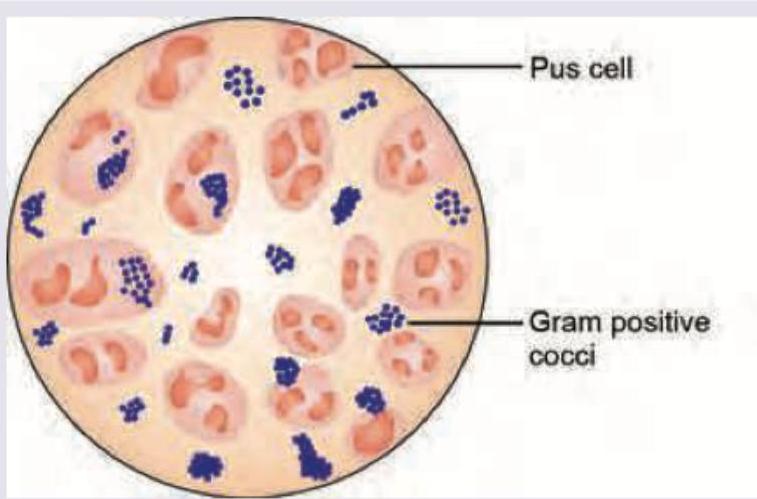
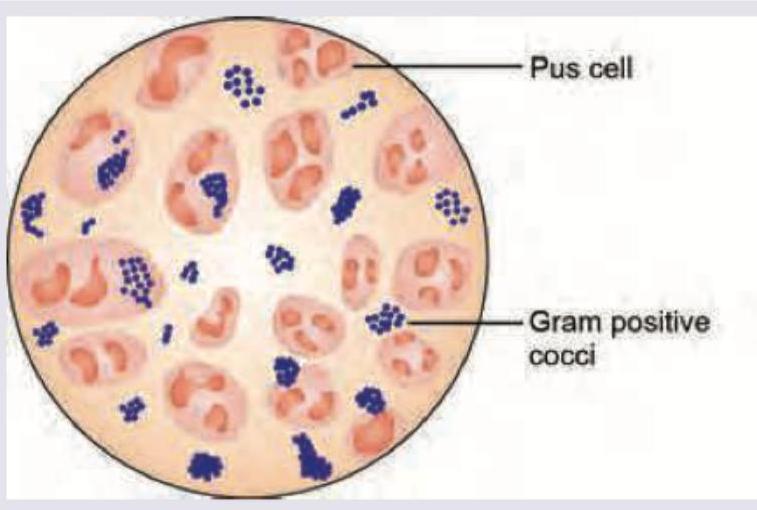
All are true about bacteria shown in the smear of pus below, except:
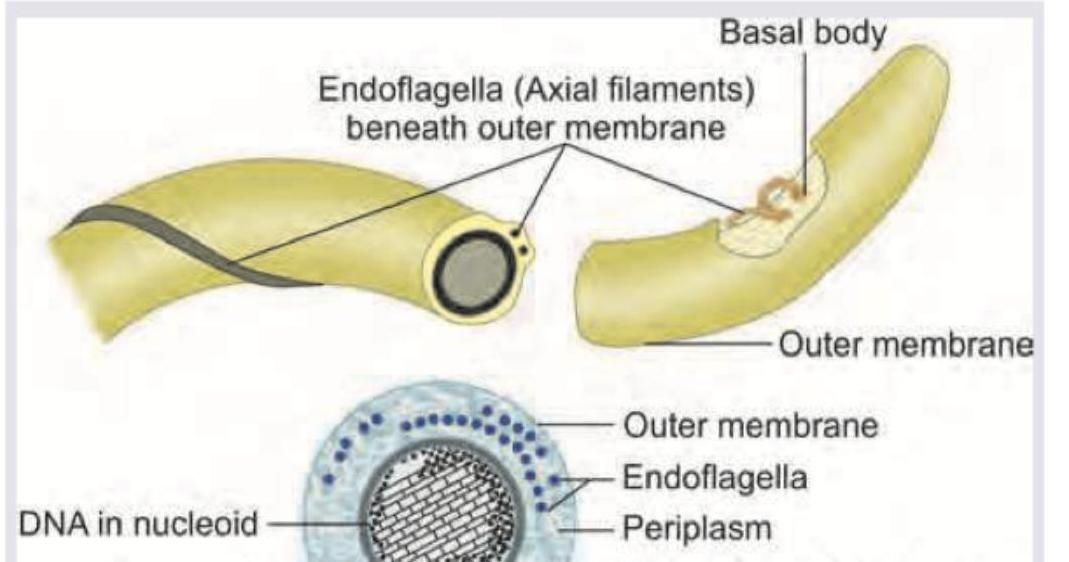
Which of the following bacteria has the flagellar characteristic shown in the image?
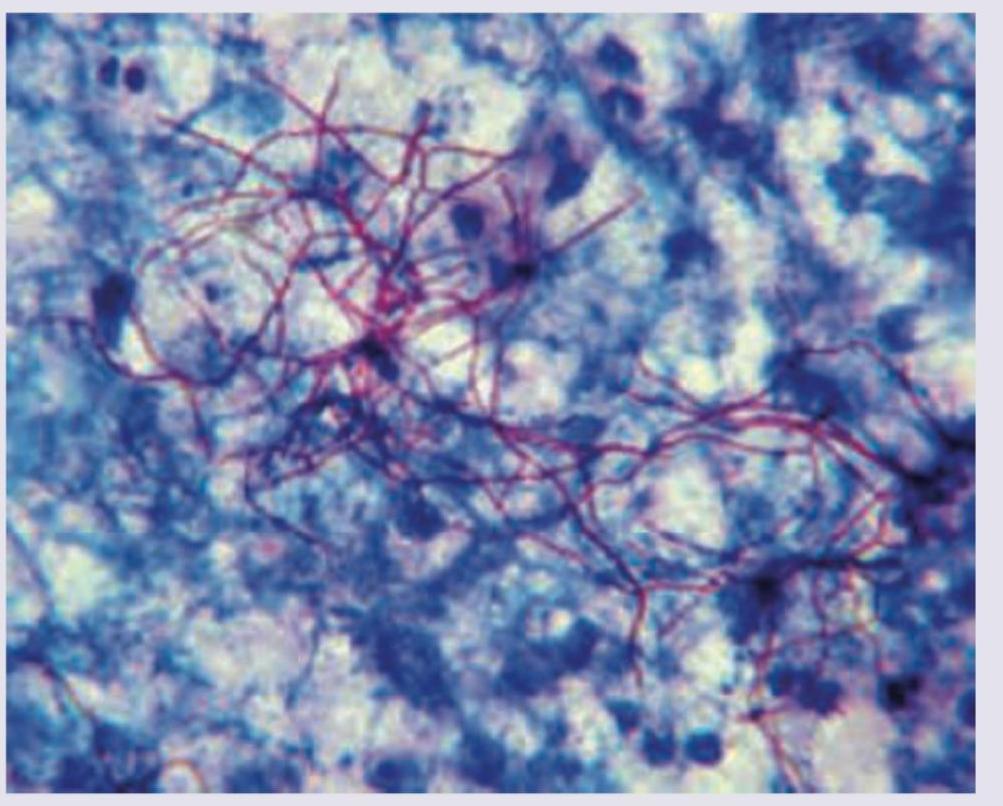
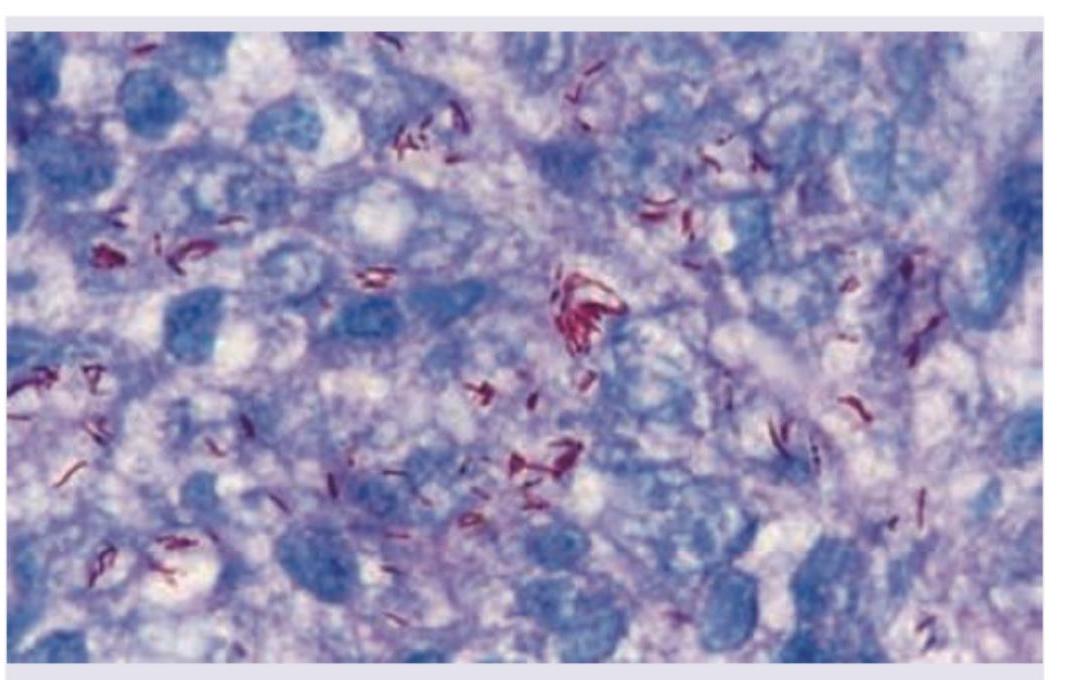
Identify the organism seen in the slide shown below.
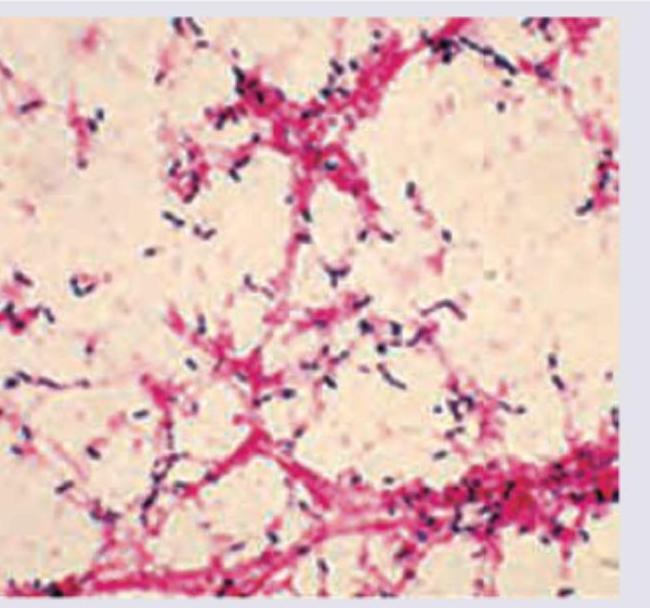
CSF gram stain of a child suffering with meningitis is shown below. What is the causative agent? (NEET Pattern 2019)
A 21-year-old college student presents with this clinical finding. All are true about the condition except:

A 13-year-old girl with cystic fibrosis has been having recurrent severe respiratory infections and transtracheal aspirate was sent for culture. The growth of pink colonies in the image shows presence of:

All are true about Helicobacter pylori on special stain preparation of stomach except:
Which of the following are the primary organisms involved in PID ? I. N. gonorrhoeae II. Chlamydia III. Mycoplasma hominis IV. Candida albicans Select the correct answer using the code given below :
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app