
Bacteriology — MCQs

On this page
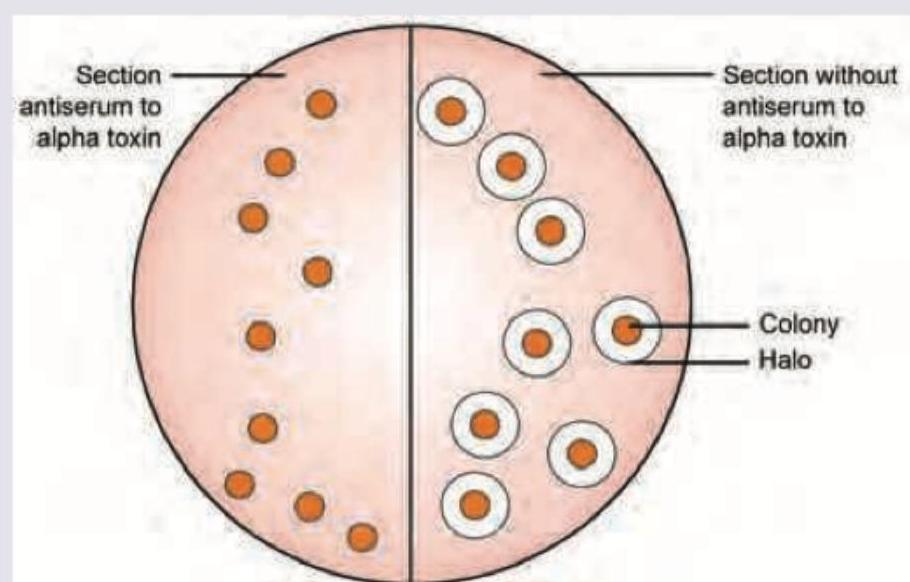
What is the following pattern seen with *Clostridium perfringens* called?
What is the drug of choice for organism producing the following colonies?
All of the following are caused by the organism shown except:
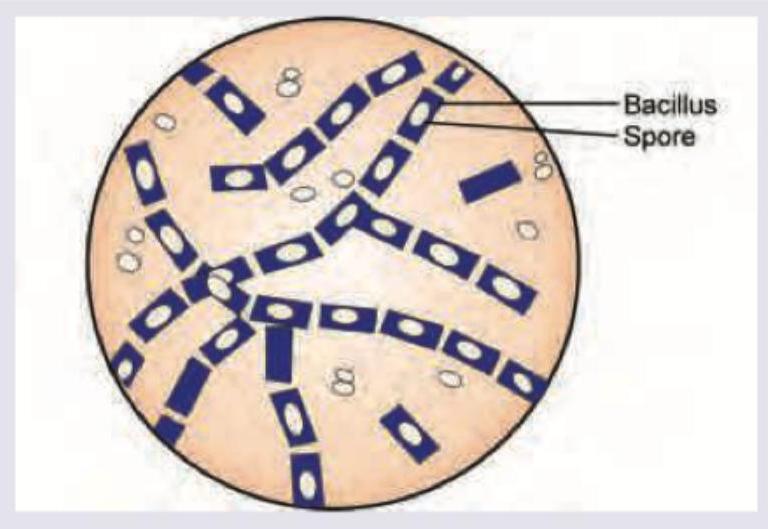
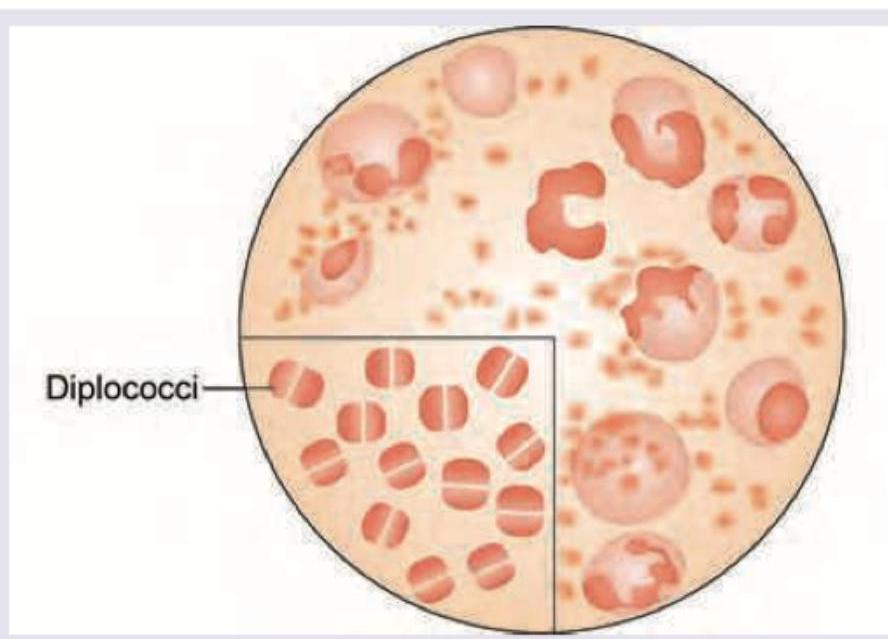
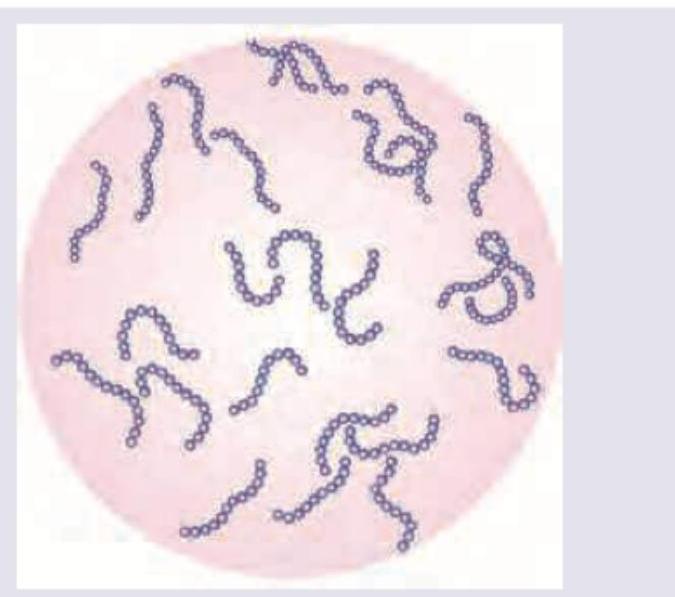
All are true about the bacteria shown except:
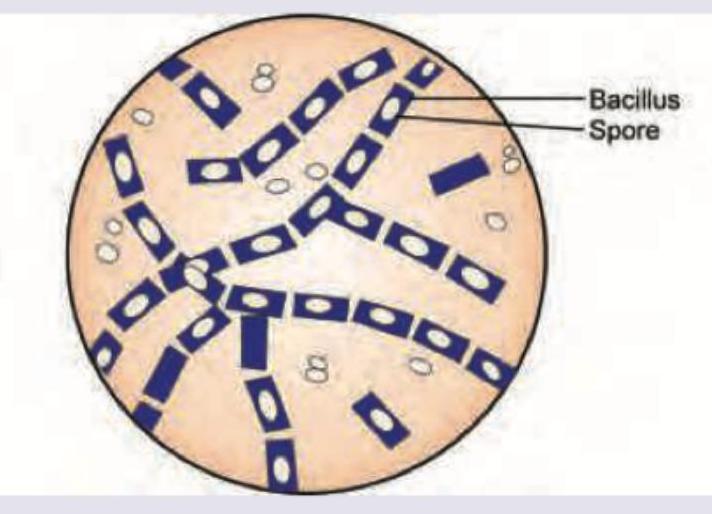
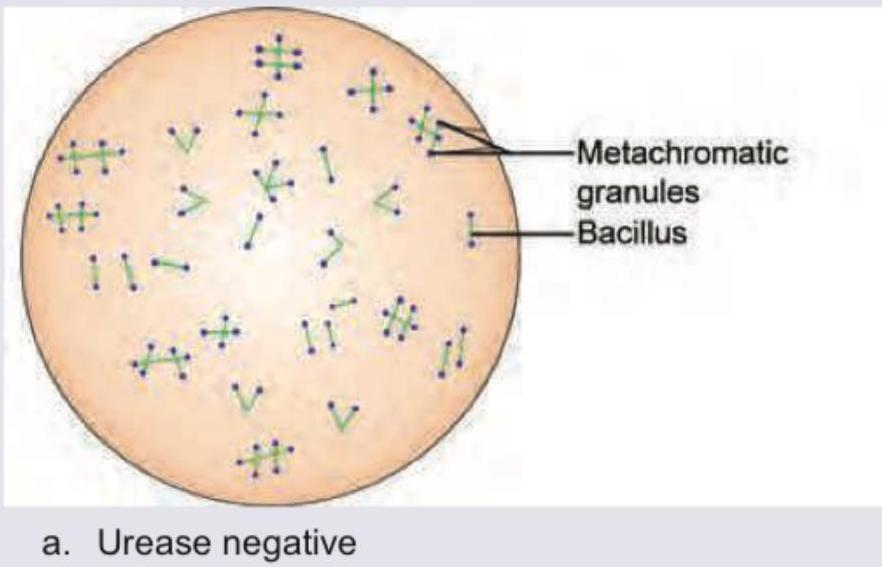
All are true about the bacteria shown in the figure except:
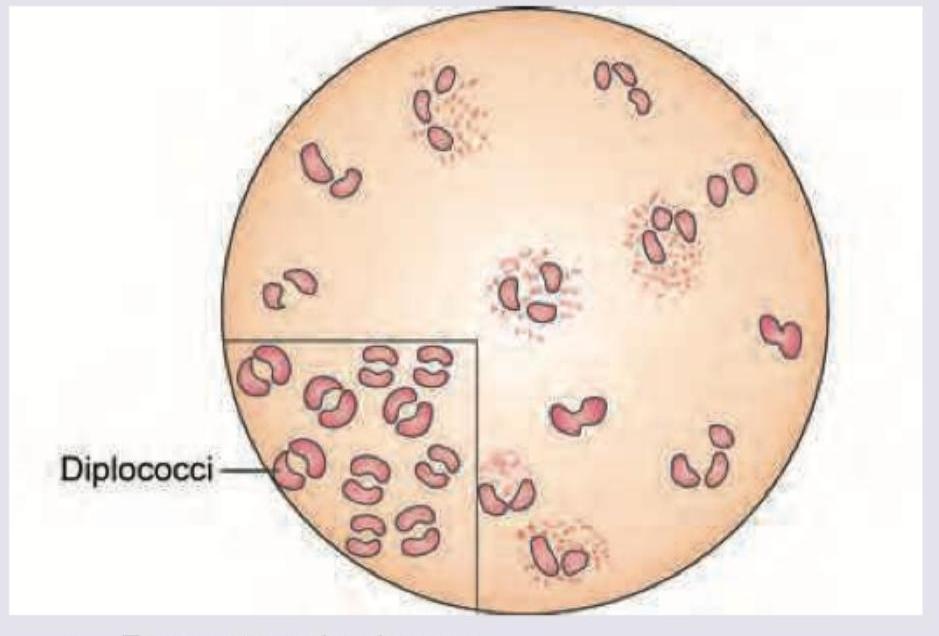
All are true about the bacteria shown in the figure except: (Recent NEET Pattern 2016-17)
All are true about the bacteria shown below except:
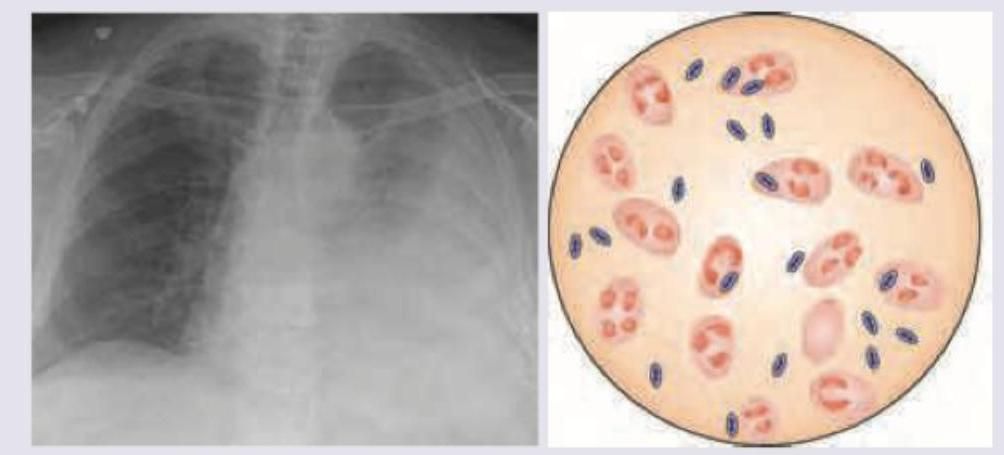
A 2-year-old child presents with fever for 5 days and fast breathing. On examination breath sounds are reduced in left infra-axillary areas and left inframammary areas. CXR was performed and pleural tap was done. Gram stain of pus drained in pleural tap shows: (Recent NEET Pattern 2016-17)
All are true about the bacteria shown below except:
Which of the following toxins will produce the condition shown below?

Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app