
Bacteriology — MCQs

On this page
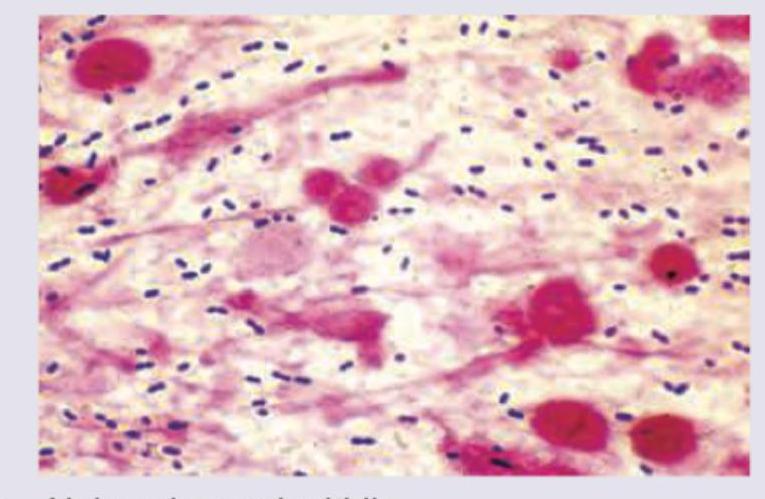
The gram stain given below shows which organism most likely? (AIIMS May 2016)
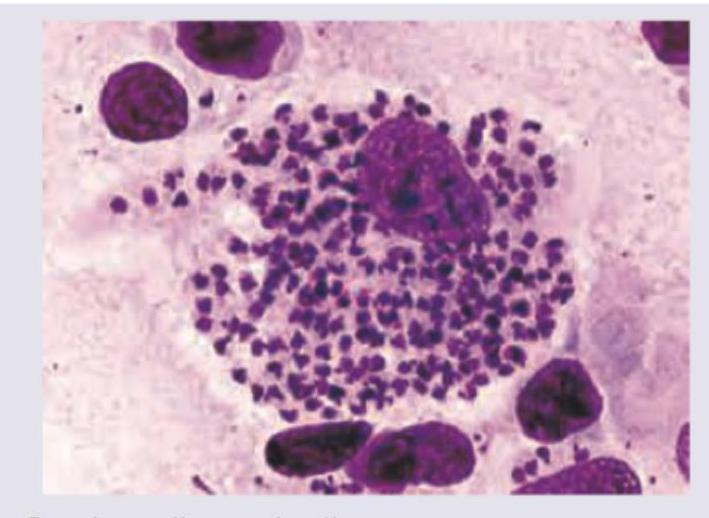
A 24-year-old female presented with an ulcer in the genital area. A Giemsa-stained tissue smear or scraping from the ulcer edge was prepared. Identify the causative agent: (AIIMS Nov 2015)
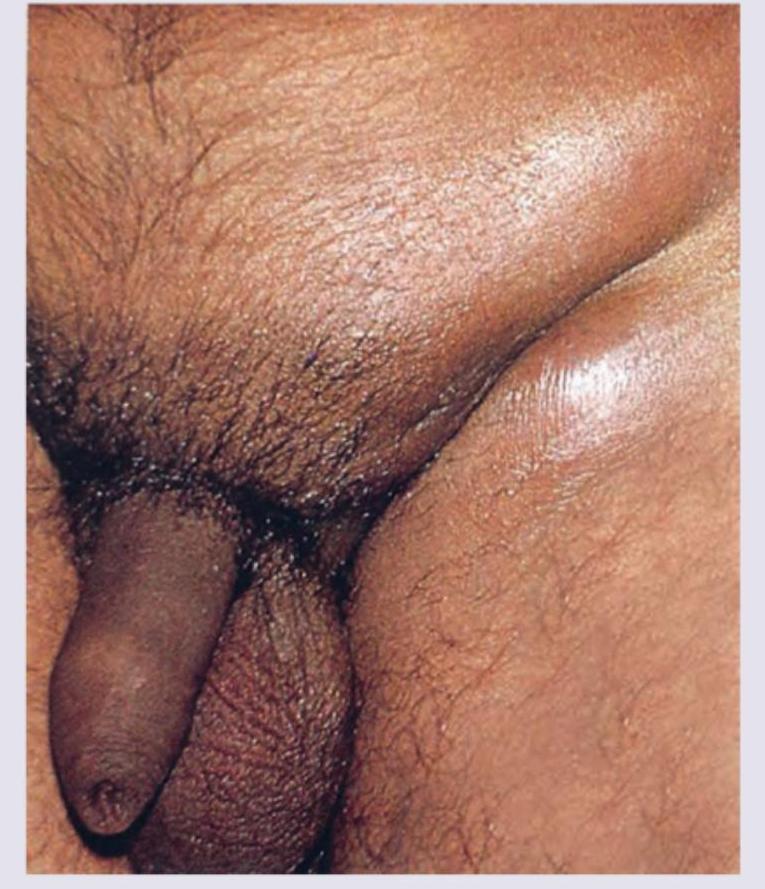
A 23-year-old female presents with fever and altered sensorium for two days with rashes on legs as shown. Her BP is 70/50 mm Hg and neck stiffness is present. Lumbar puncture reveals cloudy CSF with 4200 cells/ $\mu \mathrm{L}$, protein level 198 and glucose $21 \mathrm{mg} /$ dL. Which of the following correctly describes the organism causing this condition?

All are correct about the condition shown in the image except:
All are correct about the organism shown in the image except: (Recent NEET Pattern 2016-17)

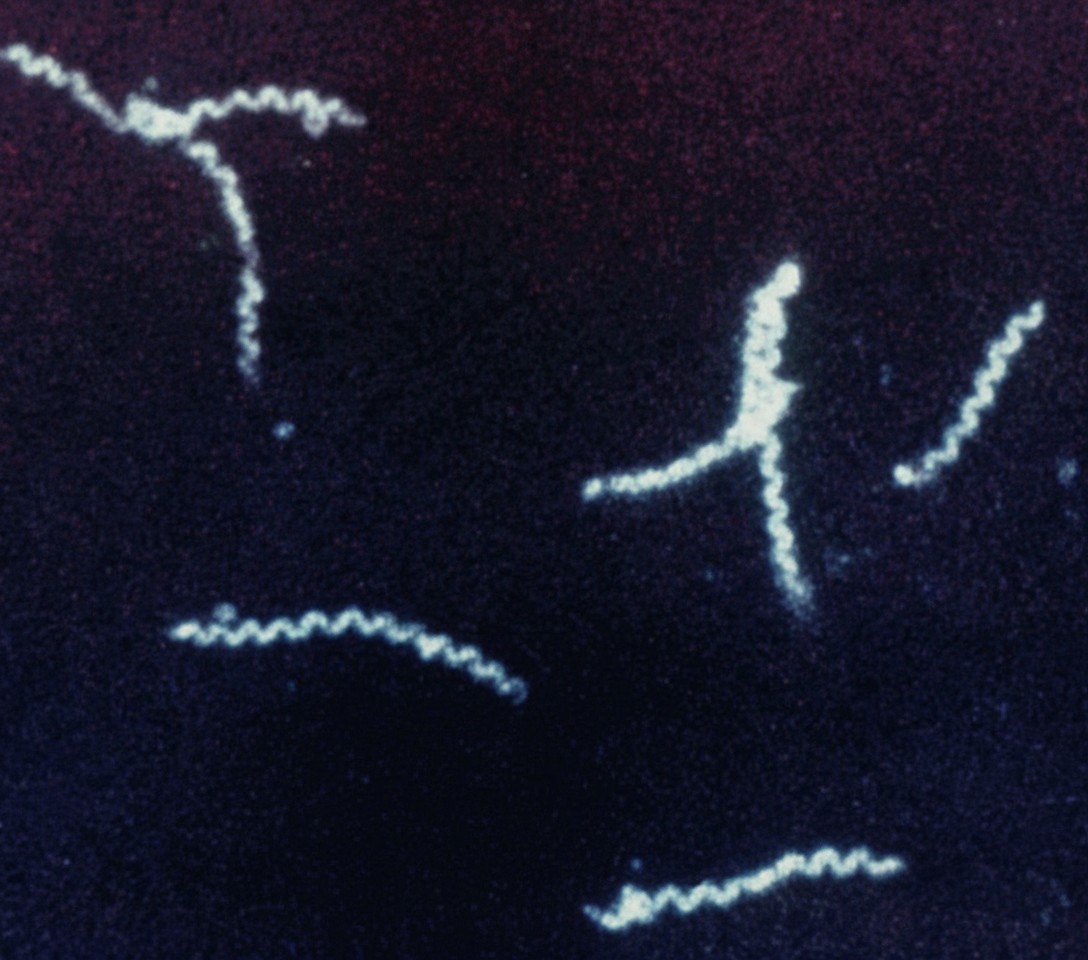
A patient presents with a painless genital ulcer (chancre). Dark-field microscopy of the lesion exudate reveals the organism shown. This organism leads to development of:
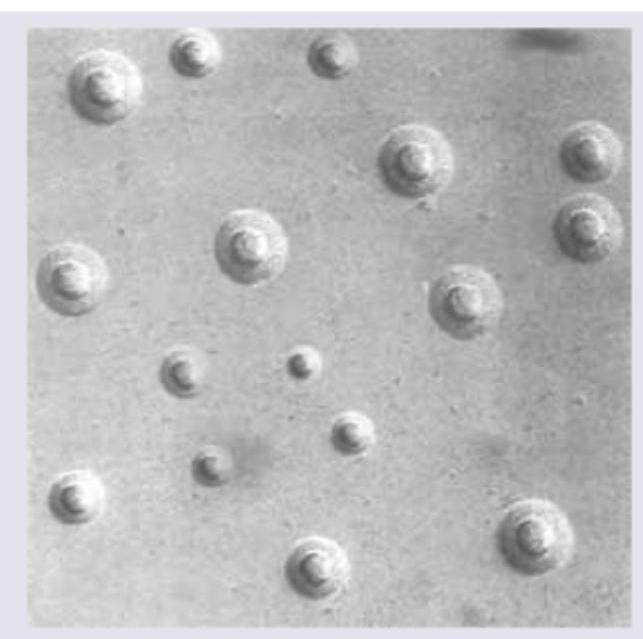
A culture from a vaginal swab grows on PPLO agar. The organism tests positive for arginine hydrolysis and negative for glucose fermentation. The following colony morphology is seen. What is the most likely organism?
A 35-year-old patient presents to the OPD 24 hours after a fight with a stranger in which he was bitten. GCS is 15/15 and following injury is noted on left forearm. He complains of extreme pain and tenderness in the injury. Swab from the injury was plated in chocolate agar and incubated in 10% carbon dioxide for 48 hours. Small colonies with pitting appearance were noted. Which of the following organism is responsible?

All are true about the organism whose colonies are shown below except:

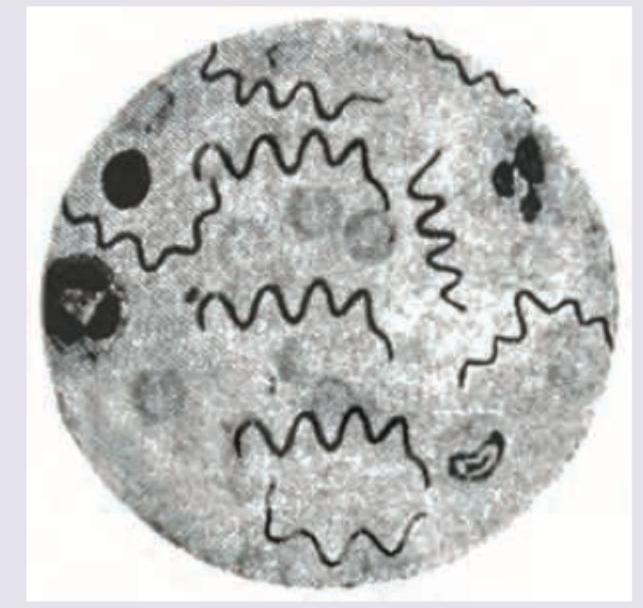
A blood smear from a patient with fever shows the following spirochetes on microscopy. Identify the organism:
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app