
Bacteriology — MCQs

On this page
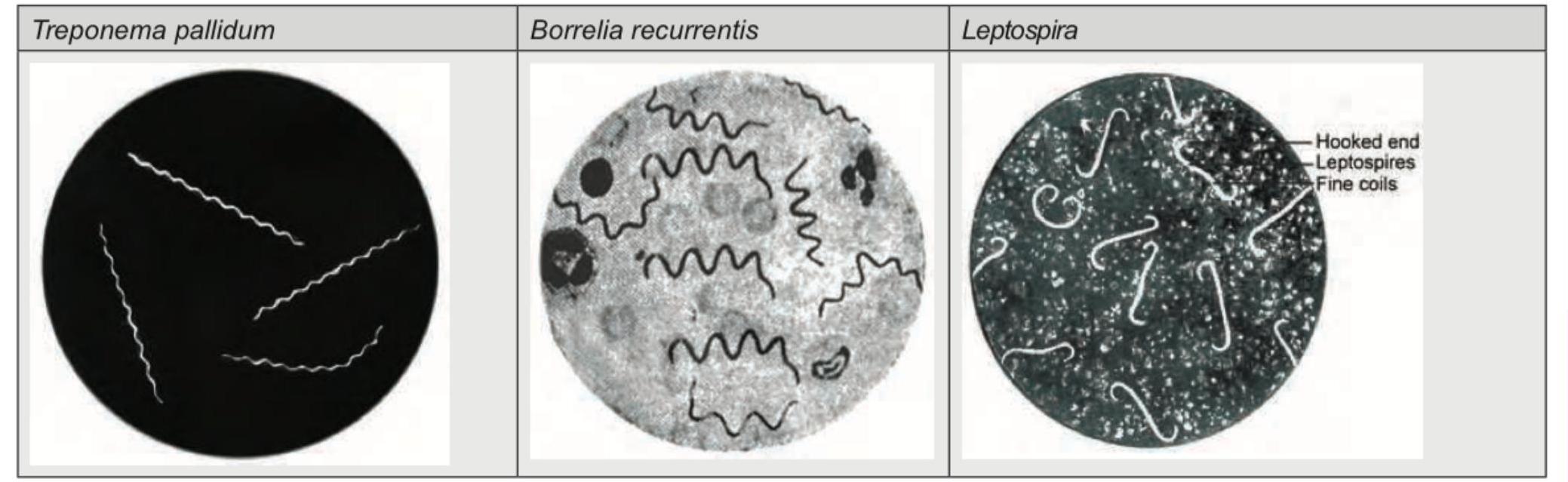
The image shows a comparison of several spirochetes. Which of the following typically has 5-8 regular spirals with hooked ends?
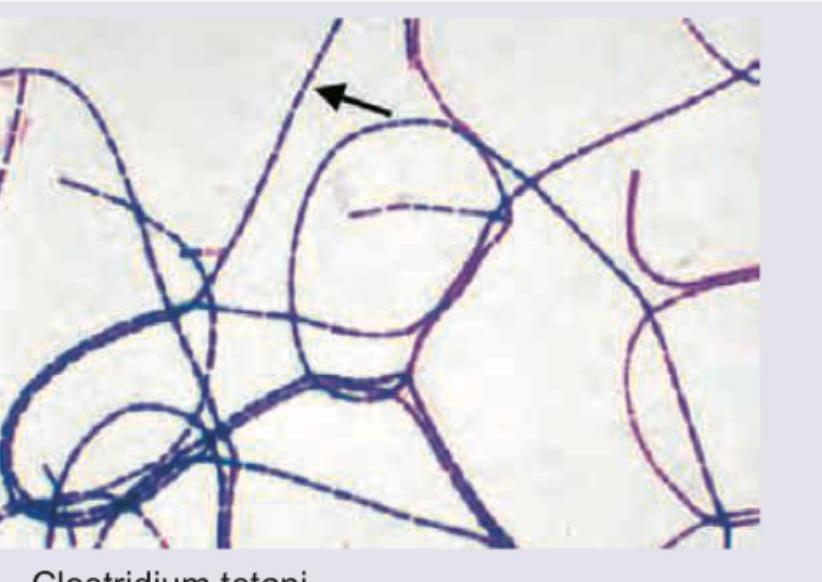
All are true about the terminal area marked 'X' in this bacteria except:

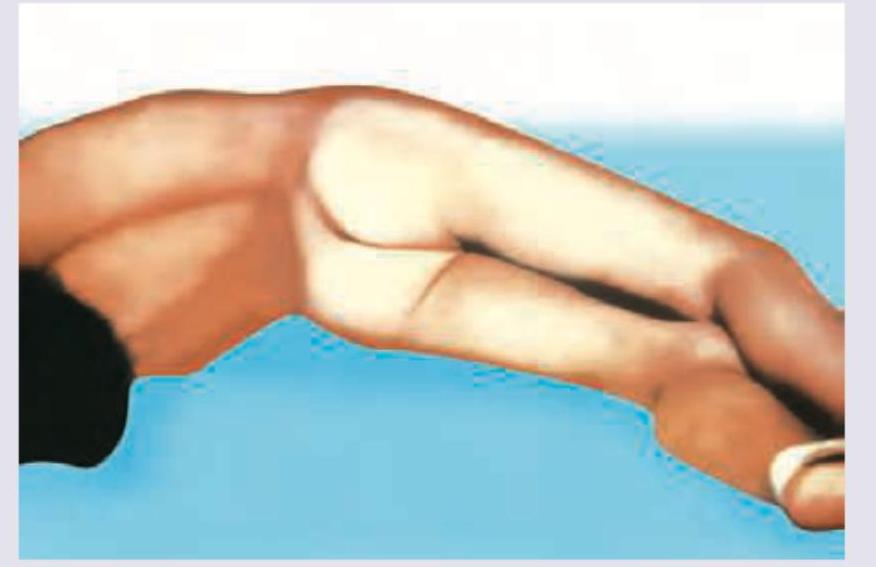
Which is incorrect about generalized tetanus shown below?
The following gram stain shows which bacteria?
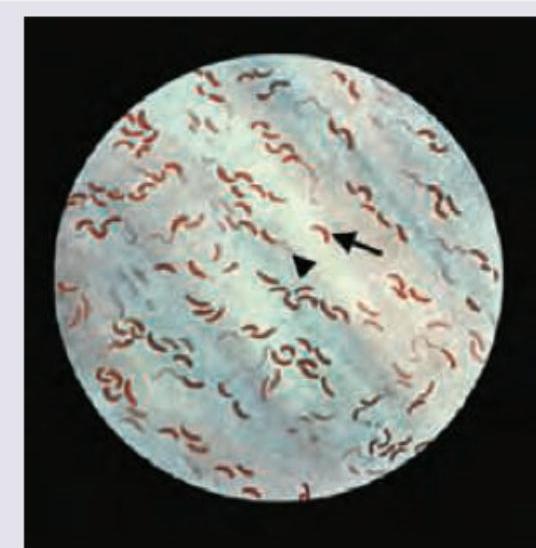
The arrow points to the presence of which bacteria?
Which of the following organisms is incriminated in a patient of left sided endocarditis involving the mitral valve? (Recent NEET Pattern 2016-17)
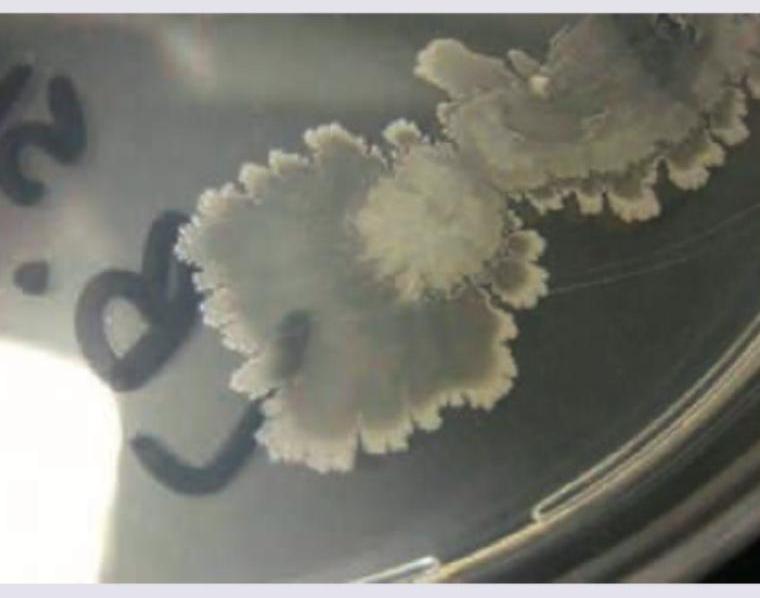
What is incorrect about the bacteria causing the following colonies? (Recent NEET Pattern 2016-17)
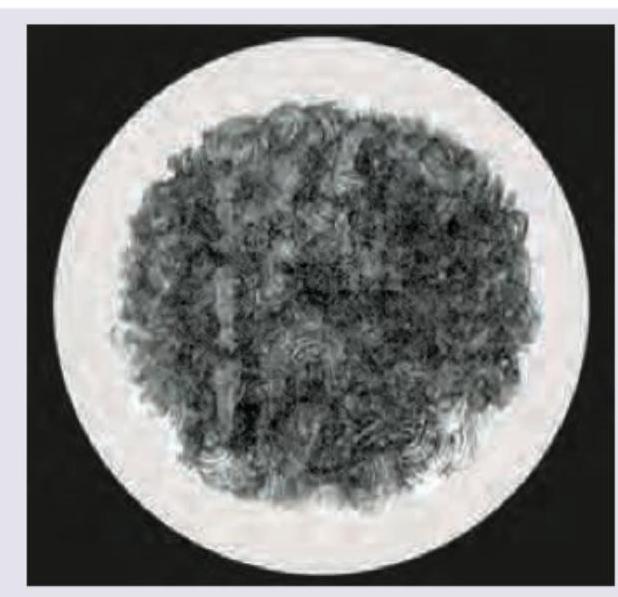
Identify the bacteria based on the colony morphology shown in the image.
Which organism is incriminated in causing the following lesions? (Recent NEET Pattern 2016-17)

A 35-year-old male farmer presents with multiple discharging cervical sinuses. Which of these stains will be useful for the diagnosis and where does this organism normally colonize in the body? (AIIMS Nov 2015)
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app