
Bacteriology — MCQs

On this page
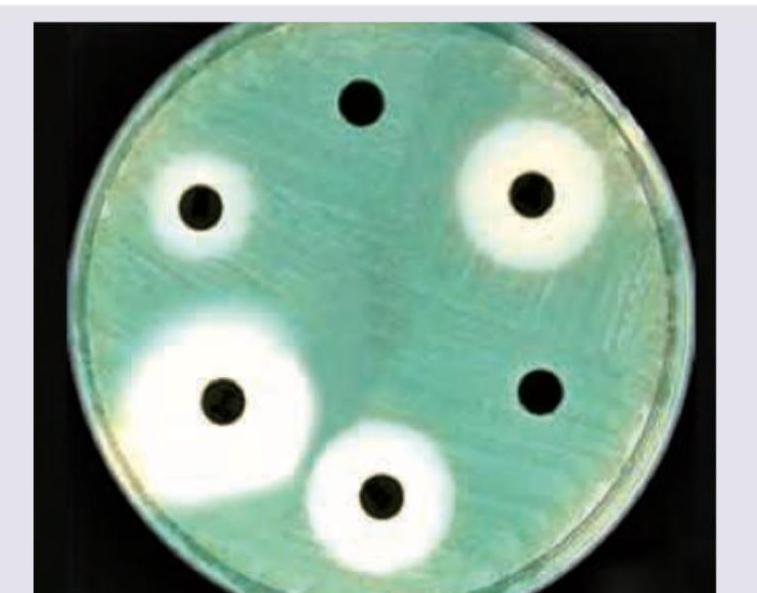
A firefighter was admitted with fever, cough, culture shown in the image reveals gram-negative, oxidase-positive bacilli. Colonies showing yellow-green fluorescence under UV light. Choose the correct agent.
A soldier presents to a referral hospital one day after sustaining a high-velocity shrapnel injury to his right thigh. He complains of severe pain at the wound site. On examination, crepitus is present. Which of the following organisms is the most likely cause of his condition?
A 70-year-old patient with a smoking history presents with high-grade fever, cough, confusion, and diarrhea. Chest X-ray shows bilateral infiltrates in bilateral lower lung fields. On sputum gram stain, no organisms were detected. Laboratory results reveal Na: 126mEq/L, AST:62, ALT:56, RBS:112 mg/dl, serum bilirubin of 0.8mg%, and a positive HIV test. Which of the following organisms is responsible?
Which of the following is an acid-fast organism?
Neutrophilic granulomatous mastitis is caused by which of the following organisms?
In a village, several people developed dysentery after consuming raw milk. On laboratory examination, gram-negative, curved rods with polymorphonuclear infiltration were found in stool samples. Which of the following is the most likely causative organism?
Group A Streptococcus is the most common cause of bacterial pharyngitis in school-aged children. Which of the following bacterial components is primarily responsible for its attachment to fibronectin on the epithelial lining of the pharynx?
A patient presents with a history of chronic meningitis. Laboratory findings show Gram-positive, filamentous branching bacteria, Positive ZN stain, Growth on paraffin bait culture. Which of the following is the most likely causative organism?
The Kanagawa phenomenon observed on Wagatsuma agar is characteristic of which of the following organisms?
Which of the following is responsible for green color on antibiotic disk sensitivity testing?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app