
Genetics and Disease — MCQs

On this page
A 40-year-old male presents with recurrent nasal polyps and asthma. Which additional condition should be screened for in this patient?
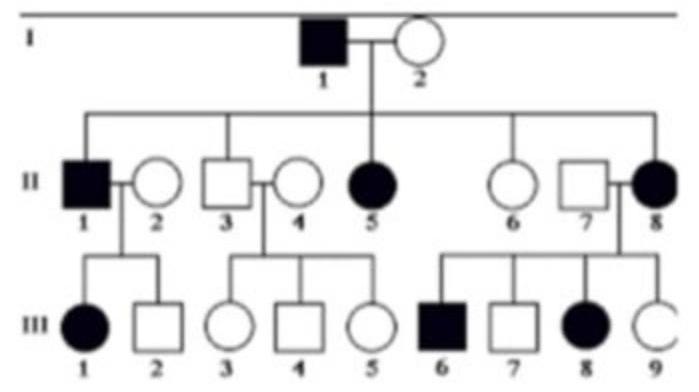
25-year-old man presents for a routine physical examination. The patient is tall and on examination, he was found to have an early diastolic murmur. His family pedigree is given below (image attached). Which of the following is the mode of inheritance by which the disease is likely to be transmitted?
In Turner's syndrome, which of the following is NOT typically observed?
Which of the following statements about Von Hippel-Lindau (VHL) syndrome is true?
Gene associated with the development of Peutz-Jeghers syndrome is?
Which of the following is NOT a feature of Abetalipoproteinemia?
Which one of the following statements is correct regarding chronic granulomatous disease (CGD)?
Following genetic counselling in a family for Familial polyposis coli (FPC), what is the next appropriate screening test for at-risk individuals?
Which karyotype is commonly associated with true hermaphroditism?
A 25-year-old man presents for a routine physical examination. He is tall and has an early diastolic murmur on examination. Based on the clinical findings, which of the following is the most likely mode of inheritance for the condition?
Practice by Chapter
Principles of Medical Genetics
Practice Questions
Genetic Testing and Counseling
Practice Questions
Single Gene Disorders
Practice Questions
Chromosomal Disorders
Practice Questions
Mitochondrial Diseases
Practice Questions
Pharmacogenomics
Practice Questions
Cancer Genetics
Practice Questions
Genetics of Common Diseases
Practice Questions
Epigenetics and Disease
Practice Questions
Genetic Basis of Developmental Disorders
Practice Questions
Ethical Issues in Medical Genetics
Practice Questions
Gene Therapy and Precision Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app