
Cardiology — MCQs

On this page
What is the initial antihypertensive agent of choice in a patient with stable ischemic heart disease?
A 40-year-old patient presents with dizziness on standing, accompanied by a systolic blood pressure reduction of 50 mm Hg. What is the appropriate treatment?
A 12-year-old boy develops cardiac symptoms attributed to rheumatic fever following a streptococcal throat infection. Years later, at age 34, he is admitted with pulmonary edema. Examination reveals a diastolic murmur at the apex, and mitral stenosis is diagnosed. Before surgical evaluation, which of the following findings can be attributed to mitral stenosis?
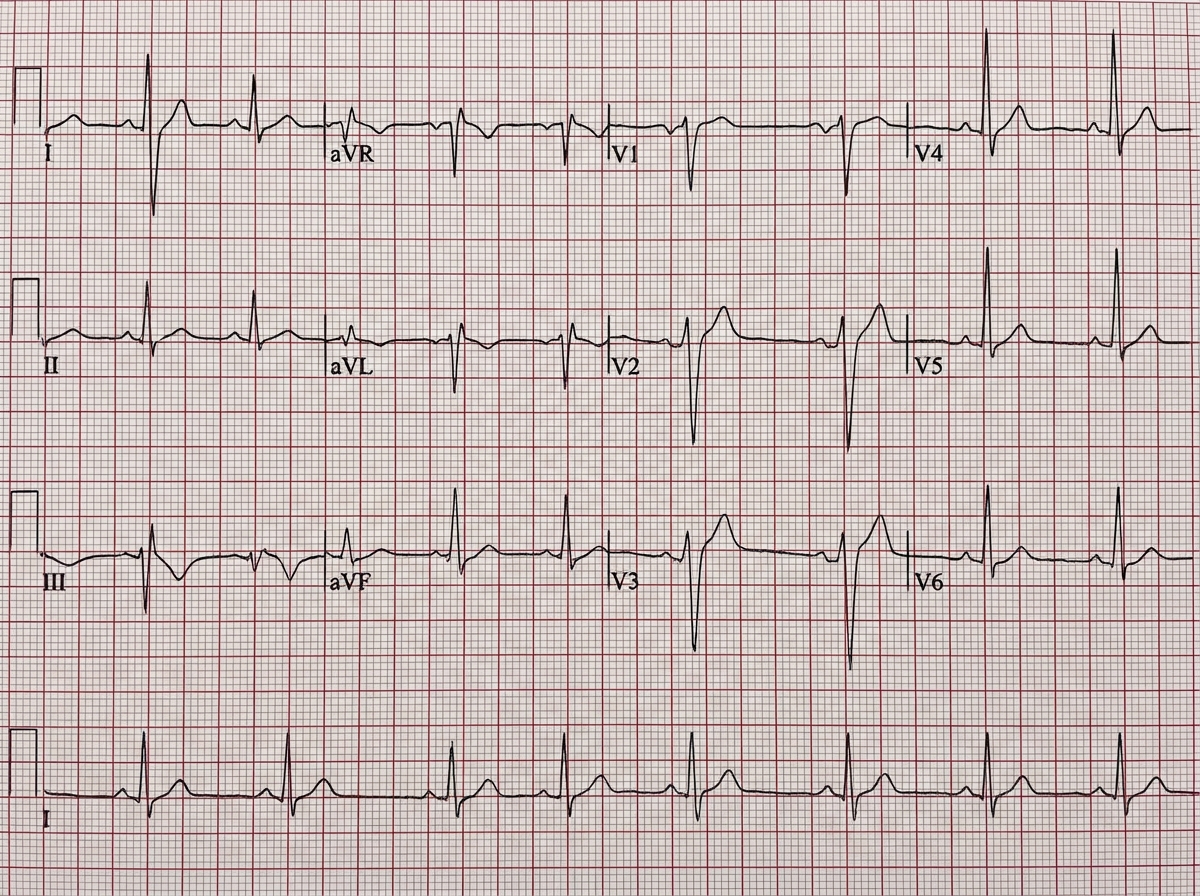
A 50-year-old lady presents to the OPD. What is the most probable diagnosis?

A 45-year-old man presents to the emergency department with sudden-onset dyspnea, pleuritic chest pain, and hypoxemia. He recently returned from a long-haul flight and has a history of deep vein thrombosis. The given ECG shows which of the following conditions?
Which of the following parameters adds predictive information regarding cardiovascular risk stratification and the measurement of serum cholesterol?
Which of the following is NOT considered a major criterion in the Framingham criteria for the diagnosis of congestive heart failure?
The right atrium chronic overload is indicated by a P wave of more than what amplitude?
Which of the following is NOT true regarding the initiation and titration of beta-blocker therapy in a patient with congestive heart failure?
All the following findings would be expected in a person with coarctation of the aorta except:
Practice by Chapter
Coronary Artery Disease and Angina
Practice Questions
Acute Coronary Syndromes
Practice Questions
Heart Failure
Practice Questions
Cardiac Arrhythmias
Practice Questions
Valvular Heart Diseases
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease in Adults
Practice Questions
Hypertension and Hypertensive Emergencies
Practice Questions
Pulmonary Hypertension
Practice Questions
Non-invasive Cardiac Diagnostics
Practice Questions
Preventive Cardiology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app