
Medicolegal Autopsies — MCQs

On this page
The following autopsy finding occurs due to:
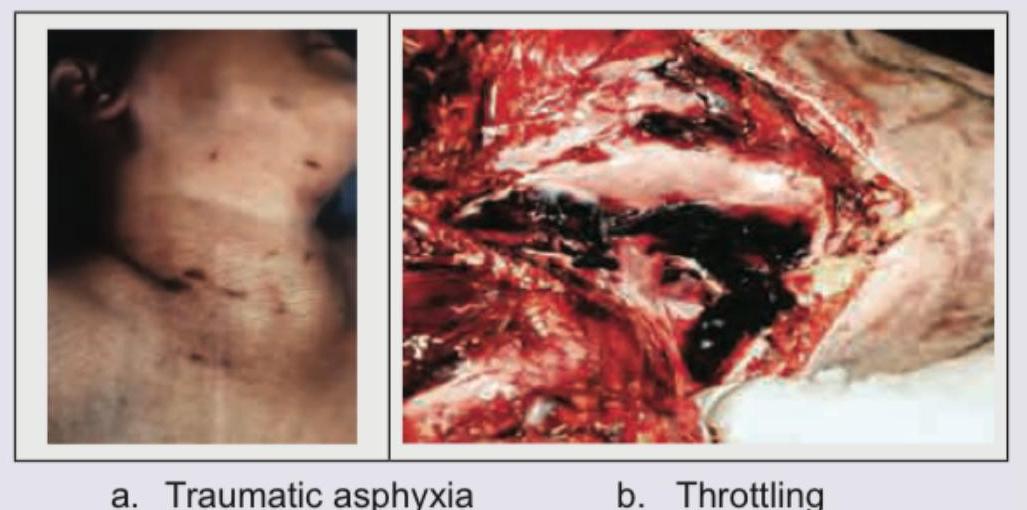
A person was brought dead to the casualty and autopsy was performed to find the cause of death. Based on the autopsy findings shown in the image, what is the diagnosis?

The following presentation is called:

A female was found dead in her bedroom. The room was not locked from inside. Her blood alcohol value was found to be 350 mg/dL. The picture taken at the post mortem is shown below. The diagnosis is? (AIIMS Nov 2018, AIIMS Nov 2017)
The clinical signs of brain-stem death include all of the following except:
In autopsy, which organ is removed with liver?
The component of vitreous humour that is most useful in determining time since death?
Certain obligations on the part of a doctor who undertakes a postmortem examination are the following, EXCEPT:
For autopsy, vitreous is preserved in:
Cardiac chambers are opened in autopsy in which order? i) Left atrium ii) Left ventricle iii) Right atrium iv) Right ventricle
Practice by Chapter
Objectives of Medicolegal Autopsy
Practice Questions
Autopsy Procedures
Practice Questions
External Examination
Practice Questions
Internal Examination
Practice Questions
Special Autopsy Techniques
Practice Questions
Organ Retention and Disposal
Practice Questions
Collection of Toxicological Samples
Practice Questions
Autopsy Report Writing
Practice Questions
Histopathology in Autopsies
Practice Questions
Microbiology in Autopsies
Practice Questions
Radiology in Autopsies
Practice Questions
Limitations and Artifacts
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app