
Phoniatrics and Voice Disorders — MCQs

On this page
What is the recommended treatment for early vocal nodules?
A 26-year-old female presents with a scratchy, croaky voice. Which of the following statements is true?
Voice produced by false vocal cords due to non-functioning of true cords is seen in which condition?
Which materials are used for injection thyroplasty?
Key nob appearance is seen in which of the following conditions?
For a case of puberphonia, which type of thyroplasty is typically used?
A 35-year-old male singer presents with complaints of hoarseness, vocal fatigue, and pain in the neck on prolonged phonation. Direct laryngoscopy shows bilateral pinhead-sized swellings on the anterior one-third and posterior two-thirds junction of the vocal cords. What is the probable diagnosis?
A patient who is a teacher by profession presents to the clinic with hoarseness of voice. What is the most likely diagnosis for this patient?
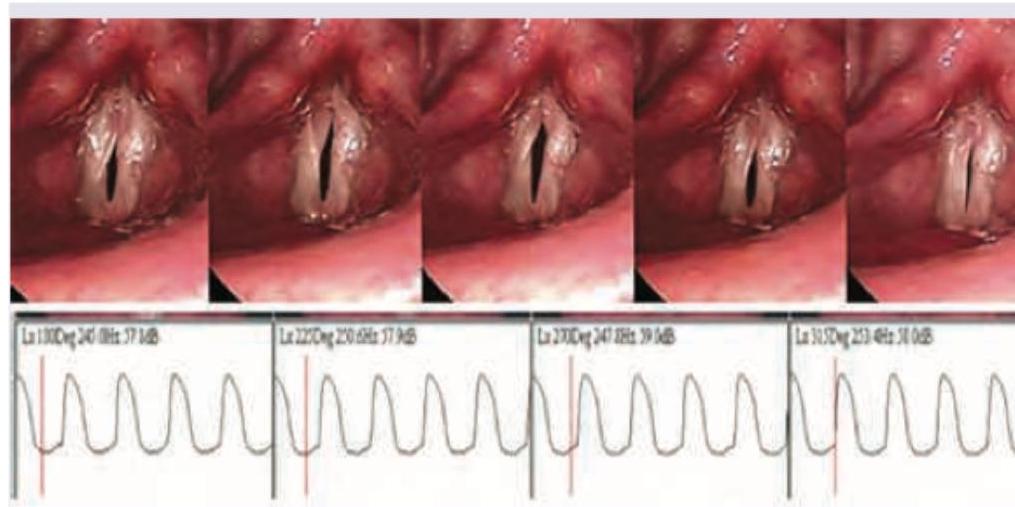
Which of the following studies is shown below?
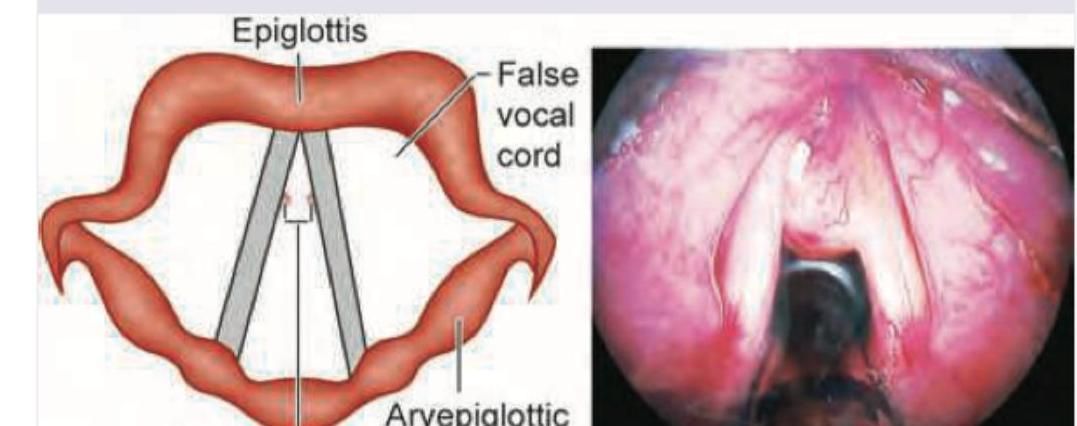
A 20-year-old lady singer of a rock band with a history of chronic vocal overuse presents with worsening diplophonia after a recent performance. The laryngoscopy image is shown below. What is the most likely diagnosis?
Practice by Chapter
Vocal Fold Structure and Function
Practice Questions
Voice Assessment and Examination
Practice Questions
Stroboscopy and High-speed Imaging
Practice Questions
Nodules, Polyps, and Cysts
Practice Questions
Vocal Fold Paralysis
Practice Questions
Spasmodic Dysphonia
Practice Questions
Professional Voice Care
Practice Questions
Voice Therapy
Practice Questions
Phonosurgery Techniques
Practice Questions
Laryngeal Framework Surgery
Practice Questions
Gender-Affirming Voice Care
Practice Questions
Pediatric Voice Disorders
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app