
Diseases of the Pharynx — MCQs

On this page
Regarding "Quinsy" all of the following are correct EXCEPT:
A 60-year-old male presents with painless cervical lymphadenopathy. On examination, the right ear reveals conductive hearing loss with a dull tympanic membrane. Moreover, decreased mobility of the soft palate was also noted. What is the probable diagnosis?
A child who underwent a tonsillectomy started bleeding while lying in the ward post-operatively. Which of the following is the most appropriate management step?
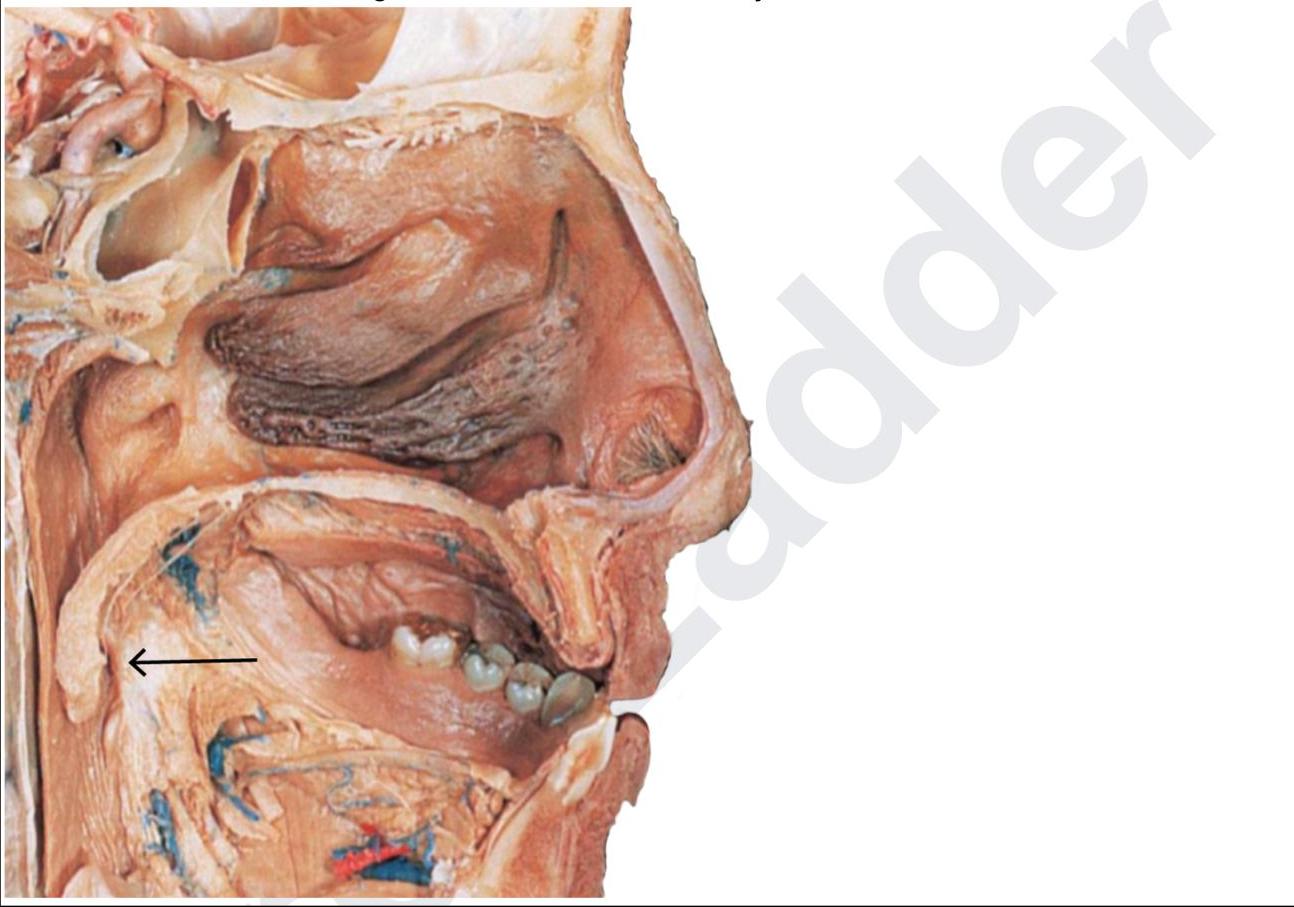
A 12-year-old presented with fever and difficulty swallowing. He had swelling in the marked region and was advised to undergo tonsillectomy. Post-surgery the gauze continued to soak with blood in a persistent, nonpulsatile venous ooze. Which of the following vessels must have been injured?
What is the most common cause of deafness in a patient with Nasopharyngeal Carcinoma:
What is the most common presentation of nasopharyngeal carcinoma?
A patient presented with 2 days history of fever. On examination there was a swelling in the neck and one side tonsil was pushed to midline. What is the most likely diagnosis:-
A 15 years old Male presented with history of fever since 2 days, unable to swallow the food with muffled voice. On examination it is noted right tonsil is shifted to midline. What is the diagnosis:
A 6-year-old boy came to the hospital with complaints of sore throat and difficulty in swallowing. His left tonsil was pushed medially and had swelling over the left side upper part of neck. What will be the diagnosis?
Angiofibroma bleeds profusely because:
Practice by Chapter
Pharyngitis
Practice Questions
Tonsillitis
Practice Questions
Peritonsillar Abscess
Practice Questions
Retropharyngeal Abscess
Practice Questions
Adenoid Hypertrophy
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Obstructive Sleep Apnea
Practice Questions
Nasopharyngeal Carcinoma
Practice Questions
Oropharyngeal Carcinoma
Practice Questions
Hypopharyngeal Carcinoma
Practice Questions
Dysphagia
Practice Questions
Globus Pharyngeus
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app