
Diseases of the Pharynx — MCQs

On this page
What is incorrect about the picture shown?

All are correct about the image shown except:

Name the instrument shown below:

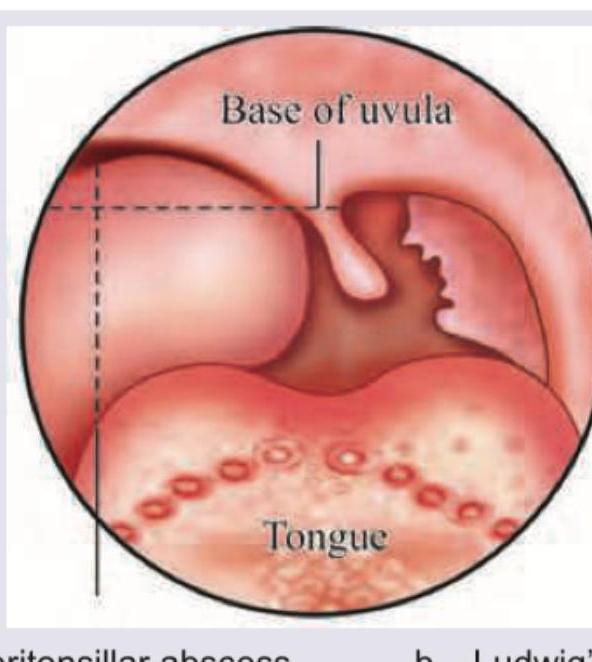
A 3-year-old child presents with fever, unilateral throat pain and trismus. Throat examination shows:
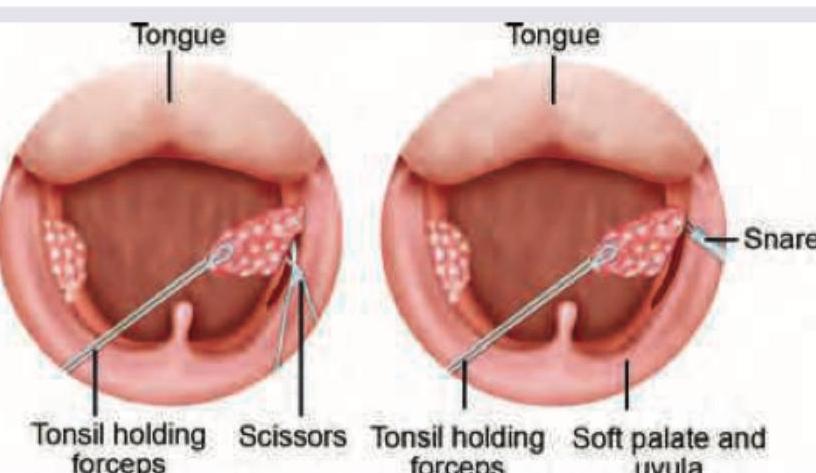
All are indications for the procedure shown except:
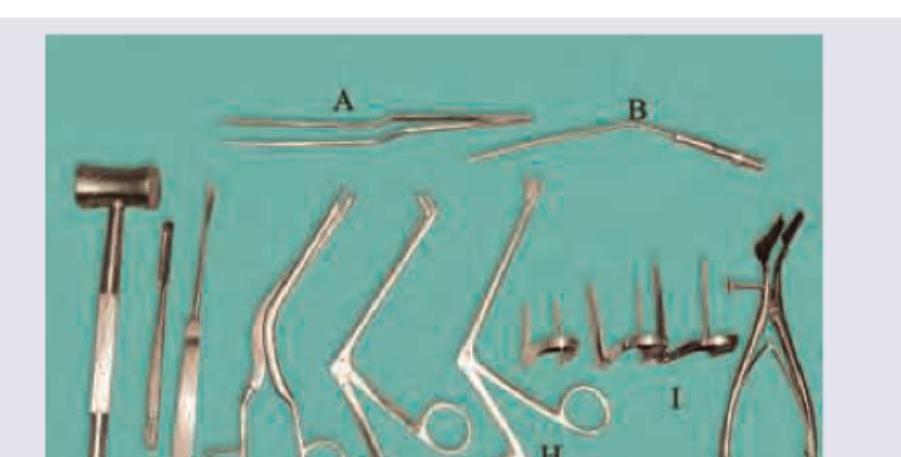
The instrument set shown below is used for performing which surgery?
A child presents with chronic nasal obstruction and mouth breathing. The facial features shown in the image are characteristic of:

Which is correct regarding the image provided?

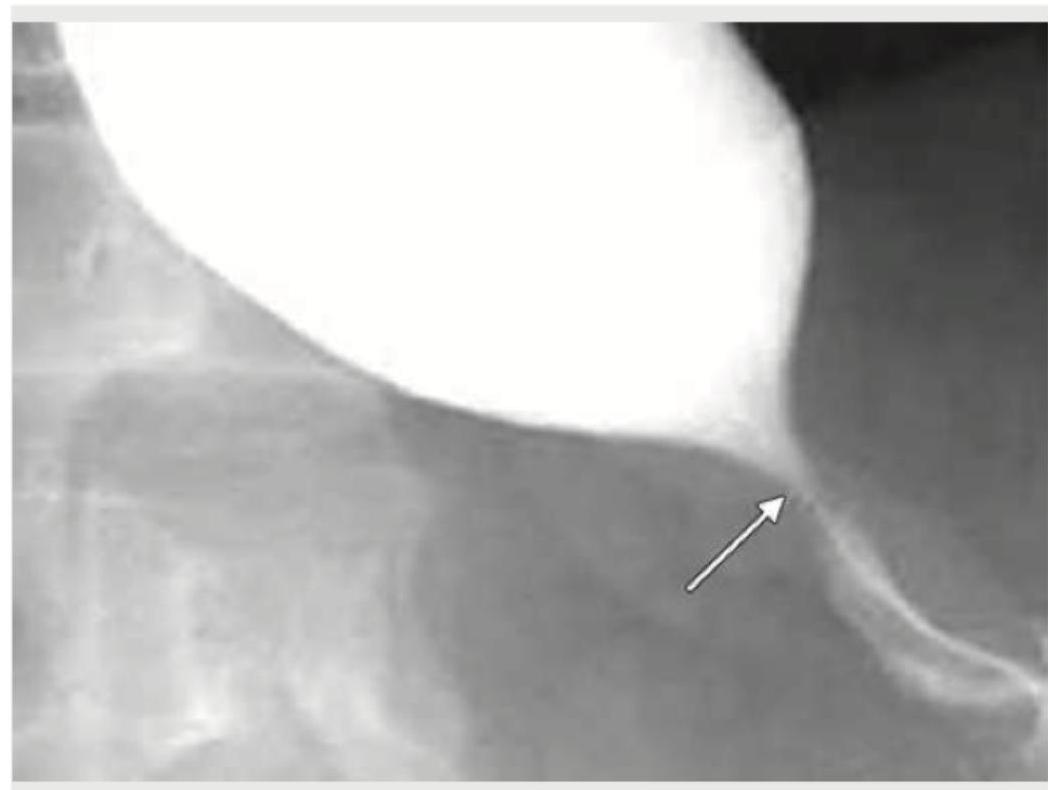
A 35-year-old woman presents with progressive dysphagia to solids, fatigue, and pallor. Laboratory workup reveals iron deficiency anemia. A barium swallow study is performed. Which of the following is true regarding the condition shown in the image?
Carcinoma of pyriform fossa usually presents with :
Practice by Chapter
Pharyngitis
Practice Questions
Tonsillitis
Practice Questions
Peritonsillar Abscess
Practice Questions
Retropharyngeal Abscess
Practice Questions
Adenoid Hypertrophy
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Obstructive Sleep Apnea
Practice Questions
Nasopharyngeal Carcinoma
Practice Questions
Oropharyngeal Carcinoma
Practice Questions
Hypopharyngeal Carcinoma
Practice Questions
Dysphagia
Practice Questions
Globus Pharyngeus
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app