
Diseases of the Pharynx — MCQs

On this page
Which age group is most commonly affected by nasopharyngeal carcinoma?
A 22-year-old male with recurrent bleeding, presents with bowing of posterior maxillary wall on CECT. All are false except?
A 50-year-old male presents with right-sided serous otitis media and a history of cervical lymphadenopathy. The probable diagnosis is?
A patient presents with a fish bone stuck in the pyriform sinus. During the removal procedure, there is accidental nerve injury. Which nerve is most likely to be damaged?
A 6-year-old child presents with recurrent episodes of sore throat, fever, and difficulty swallowing for the past 2 years, with 7 documented episodes in the last year. Examination reveals enlarged, inflamed tonsils with exudate. The child has missed significant school days. What is the most appropriate management?
Which of the following is incorrect regarding Juvenile Nasopharyngeal Angiofibroma (JNA)?
A 12-year-old male with a history of recurrent epistaxis presents with nasal obstruction for the past 1 year. On examination the presence of nasal mass and investigation shows bowing of the posterior wall of maxillary sinus. What is the probable diagnosis?
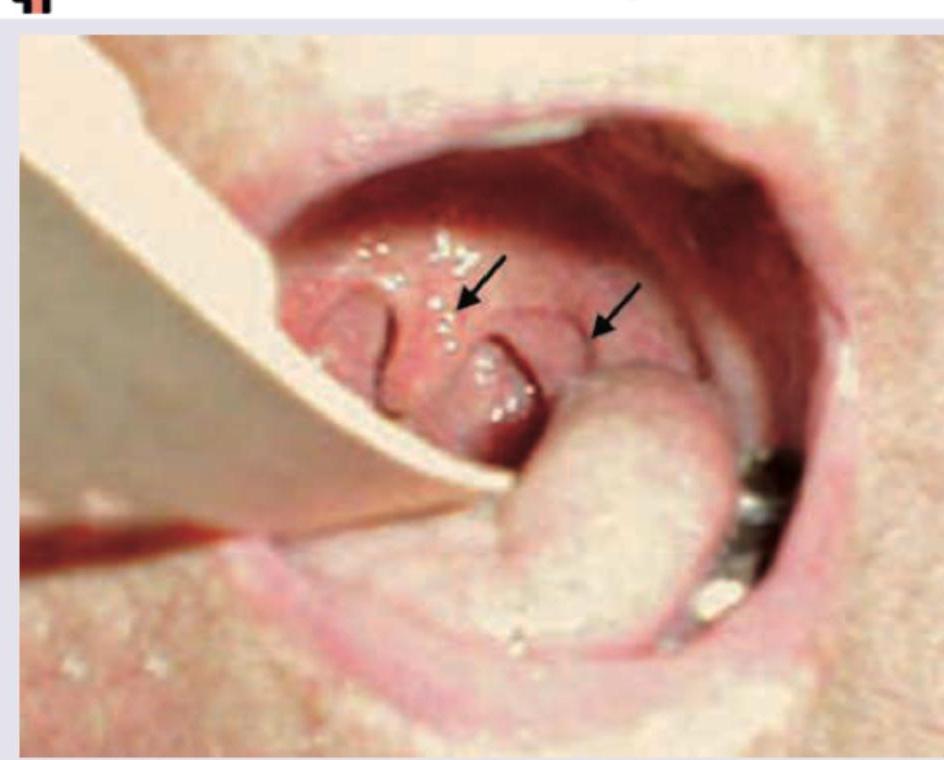
All are correct about the image shown below except:
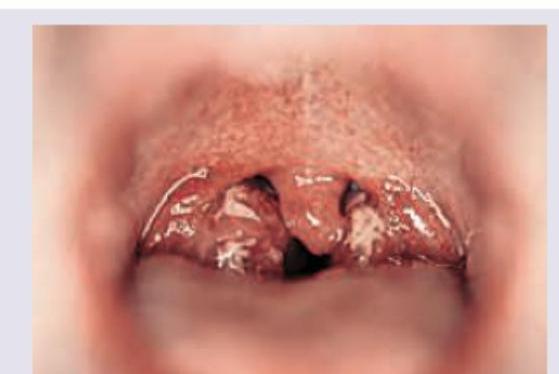
All are correct about the condition except:
Which is incorrect about the instrument shown?

Practice by Chapter
Pharyngitis
Practice Questions
Tonsillitis
Practice Questions
Peritonsillar Abscess
Practice Questions
Retropharyngeal Abscess
Practice Questions
Adenoid Hypertrophy
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Obstructive Sleep Apnea
Practice Questions
Nasopharyngeal Carcinoma
Practice Questions
Oropharyngeal Carcinoma
Practice Questions
Hypopharyngeal Carcinoma
Practice Questions
Dysphagia
Practice Questions
Globus Pharyngeus
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app