
Diseases of the Pharynx — MCQs

On this page
All of the following are true about Thornwaldt's abscess except?
An 80-year-old female presents with complaints of difficulty swallowing and foul breath for 4 months. On auscultation, her lung fields have crepitations. A barium swallow finding is shown. What is your diagnosis?

Which of the following statements is NOT true about Glossopharyngeal neuralgia?
Hot potato voice is seen in all of the following conditions EXCEPT:
Which of the following statements is true regarding Plummer-Vinson syndrome?
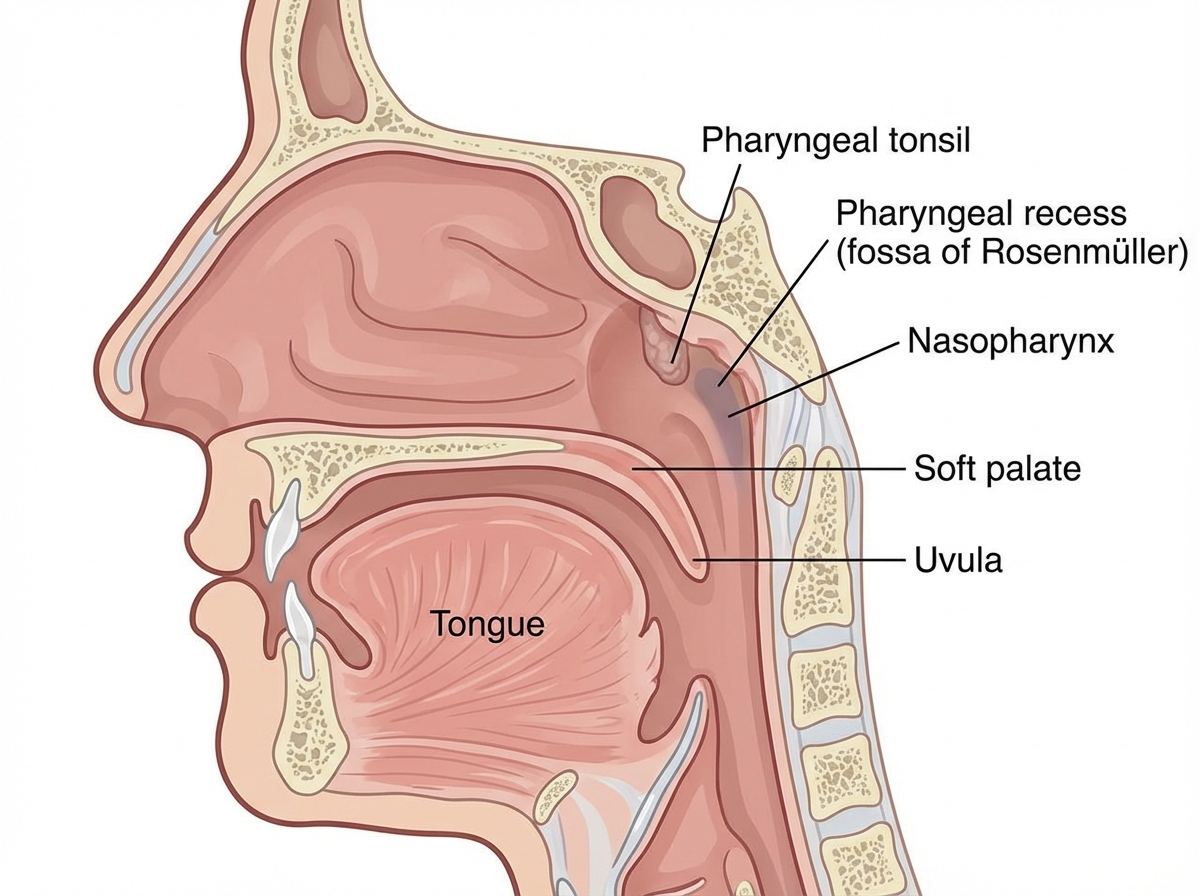
A marked area in the nasopharynx gives rise to which of the following diseases?
The association of membranous tonsillitis with petechial eruption on the palate and generalized lymphadenopathy should suggest which diagnosis?
A 70-year-old man presents with regurgitation of food, dysphagia, halitosis, and a sensation of 'lump in the throat'. What is the most likely diagnosis?
Anti-gravity aspiration is done in which of the following conditions?
Radiotherapy is used in the treatment of angiofibroma when it involves which of the following structures?
Practice by Chapter
Pharyngitis
Practice Questions
Tonsillitis
Practice Questions
Peritonsillar Abscess
Practice Questions
Retropharyngeal Abscess
Practice Questions
Adenoid Hypertrophy
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Obstructive Sleep Apnea
Practice Questions
Nasopharyngeal Carcinoma
Practice Questions
Oropharyngeal Carcinoma
Practice Questions
Hypopharyngeal Carcinoma
Practice Questions
Dysphagia
Practice Questions
Globus Pharyngeus
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app