
Diseases of the Pharynx — MCQs

On this page
A 4-year-old male presents with recurrent upper respiratory tract infections, difficulty breathing, high arched palate, failure to grow, and impaired hearing. What is the most appropriate management?
Trotter's triad is seen in which of the following conditions?
A 74-year-old male complains of bad breath, regurgitation of food during his sleep, and weight loss. For several months he has also had trouble swallowing solids. He denies fever, chills, and nausea. The patient does not smoke cigarettes and does not drink alcohol. Barium swallow study with fluoroscopy is obtained. Which of the following is the most likely underlying cause of the patient's condition?
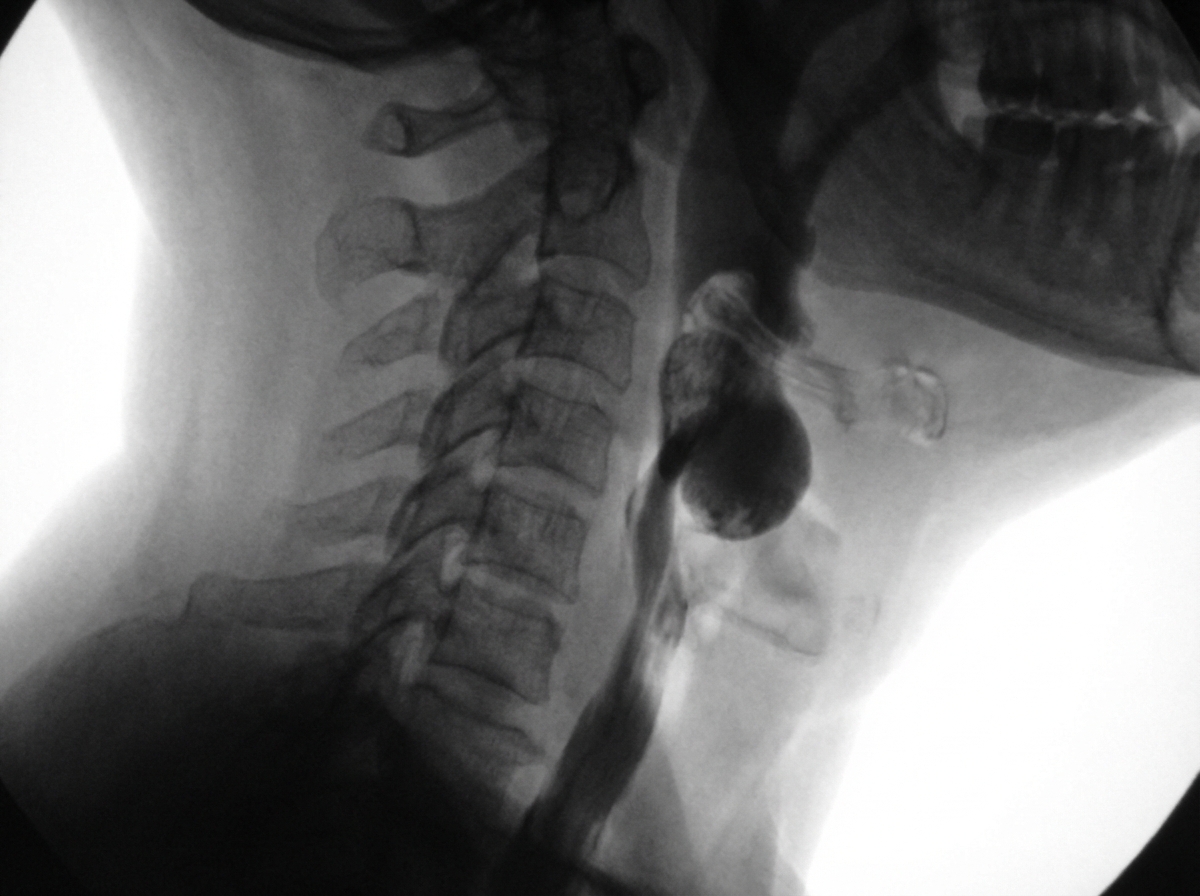
All of the following are true about Zenker's Diverticulum except?
A patient presents with unilateral throat pain worsened by swallowing, dysphagia, and a foreign-body sensation in the throat. The X-ray shown below is diagnostic of what? The finding in the X-ray is marked with a red arrow.

Which of the following is called the gateway of Tears?
What is not characteristic of Eagle's syndrome?
Which of the following is not a complication of adenoidectomy?
Which of the following is NOT a feature of Plummer-Vinson syndrome?
A child presented to the OPD with fever and dysphagia. On examination, the following was visualized. What is your most probable diagnosis?

Practice by Chapter
Pharyngitis
Practice Questions
Tonsillitis
Practice Questions
Peritonsillar Abscess
Practice Questions
Retropharyngeal Abscess
Practice Questions
Adenoid Hypertrophy
Practice Questions
Sleep-Disordered Breathing
Practice Questions
Obstructive Sleep Apnea
Practice Questions
Nasopharyngeal Carcinoma
Practice Questions
Oropharyngeal Carcinoma
Practice Questions
Hypopharyngeal Carcinoma
Practice Questions
Dysphagia
Practice Questions
Globus Pharyngeus
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app