
Fungal Skin Infections — MCQs

On this page
The image shows a KOH mount suggestive of diagnosis of:
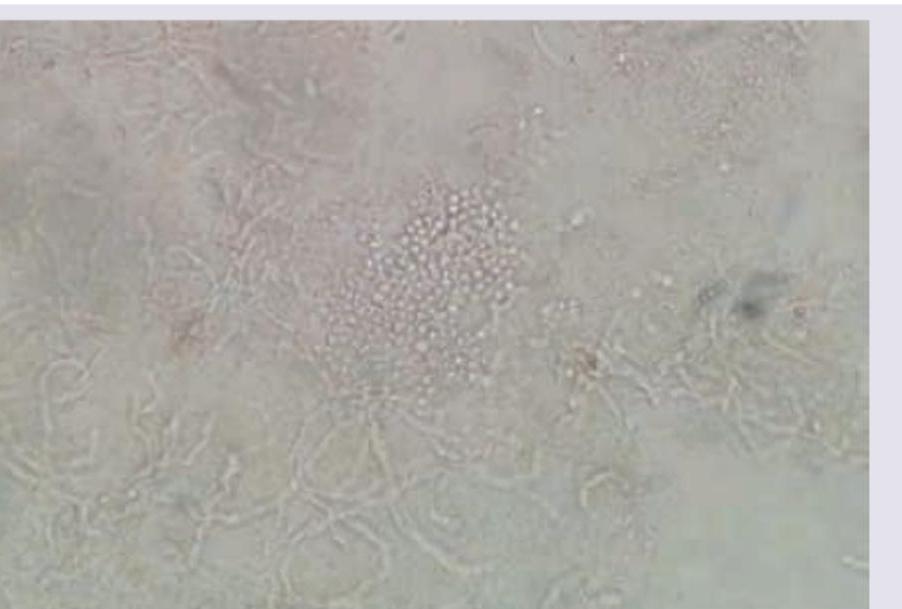
Which of the following is not effective against this condition?

All are true about the image shown except:
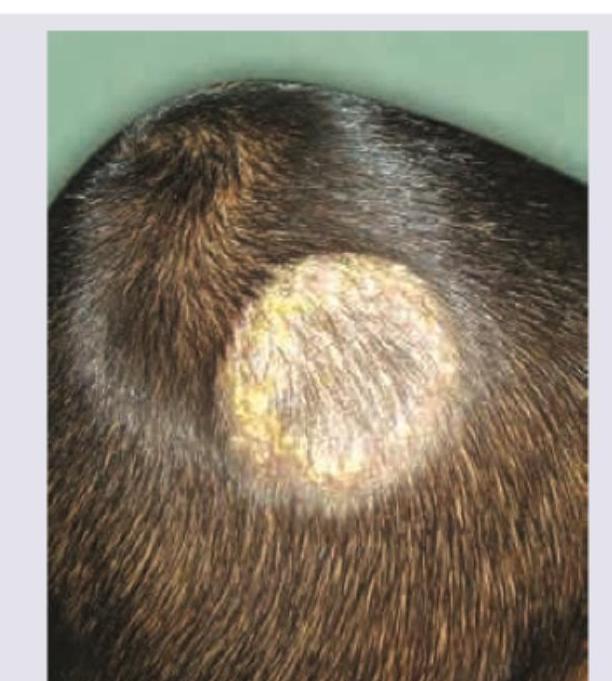
The cup-shaped yellow crusts shown in the image are called:
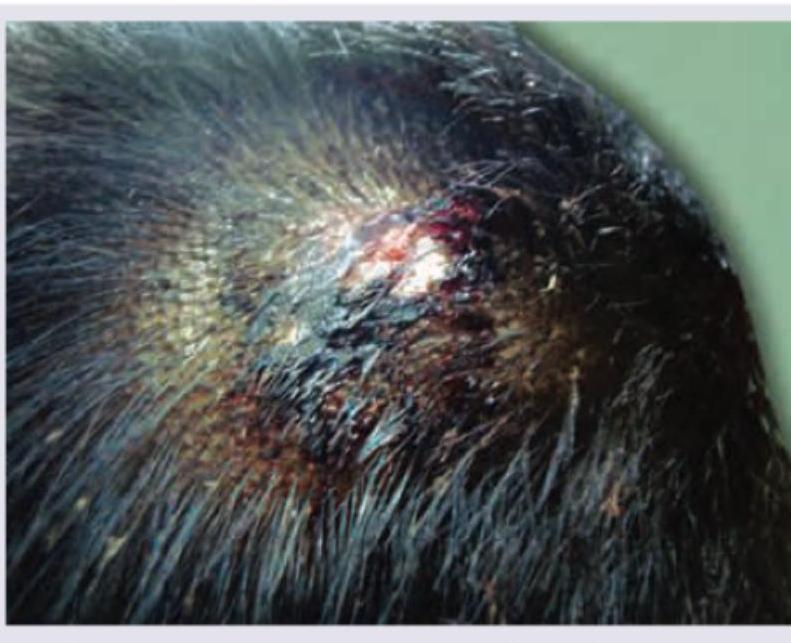
A child has been brought with the following scalp lesion with history of itching in scalp and hair loss for past 2 months. Which of the following is useful for diagnosis of this patient? (AIIMS May 2017)

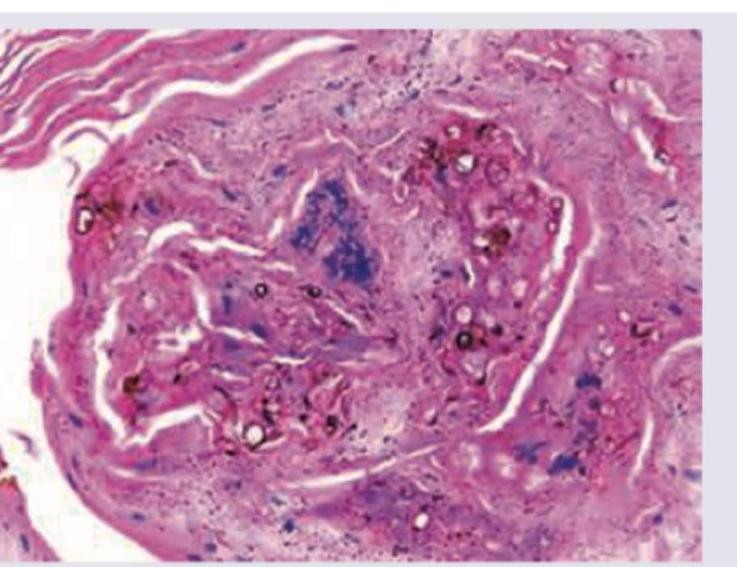
A 35-year-old presented with a single warty lesion on the foot after a thorn prick. No regional lymph nodes are seen. Biopsy shows the following lesion. Diagnosis is:
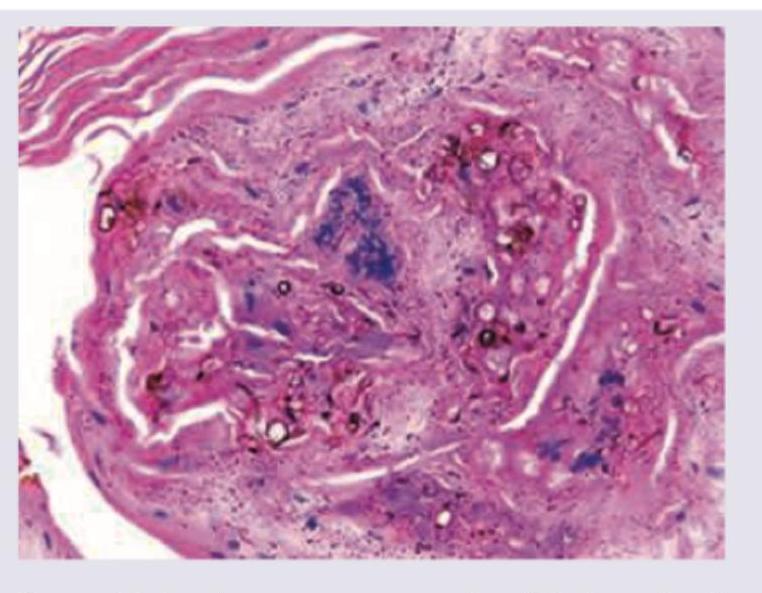
A 35-year-old presented with a single warty lesion on the foot after a thorn prick. No regional lymph nodes are seen. Biopsy shows the following lesion. Treatment is?
Which of the following is the most appropriate treatment for the skin condition shown in the image?

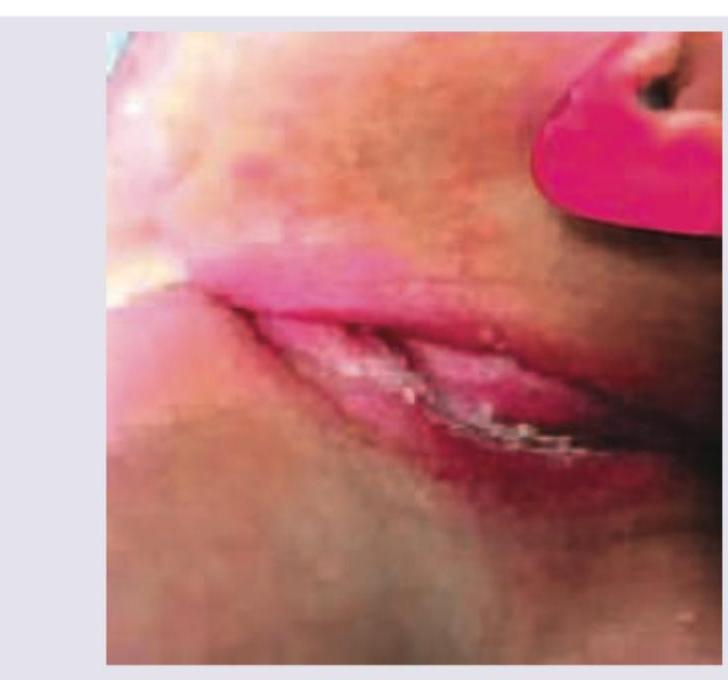
What is the diagnosis of the lesion visible in neck folds of this child?
A 56 year old gardener presents with an ulcerative nodule with purulent discharge on his right index finger. He had a prick with a thorn, at the same site around a month back. Which one of the following infections is most likely?
Practice by Chapter
Dermatophytoses
Practice Questions
Tinea Versicolor
Practice Questions
Candidiasis
Practice Questions
Onychomycosis
Practice Questions
Subcutaneous Mycoses
Practice Questions
Systemic Mycoses with Cutaneous Manifestations
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Mycetoma
Practice Questions
Tropical Fungal Infections
Practice Questions
Diagnosis of Fungal Infections
Practice Questions
Antifungal Therapy
Practice Questions
Preventive Strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app