
Fungal Skin Infections — MCQs

On this page
All of the following statements regarding this image are true except: (Recent NEET Pattern 2016-17)

A 42-year-old male complains of itching, his clinical presentation is given in the image. Which of the following statement is false?

A 25-year-woman developed scaly, pruritic lesions on her back. She applied topical steroids on the lesion, following the advice of a quack. Subsequently her lesions worsened. What is the diagnosis?
The given picture depicts:

A 30-year-old washerwoman presents with the following lesion. All are correct except:

A 20-year-old patient presents with an extremely itchy lesion on one arm. Diagnosis is:

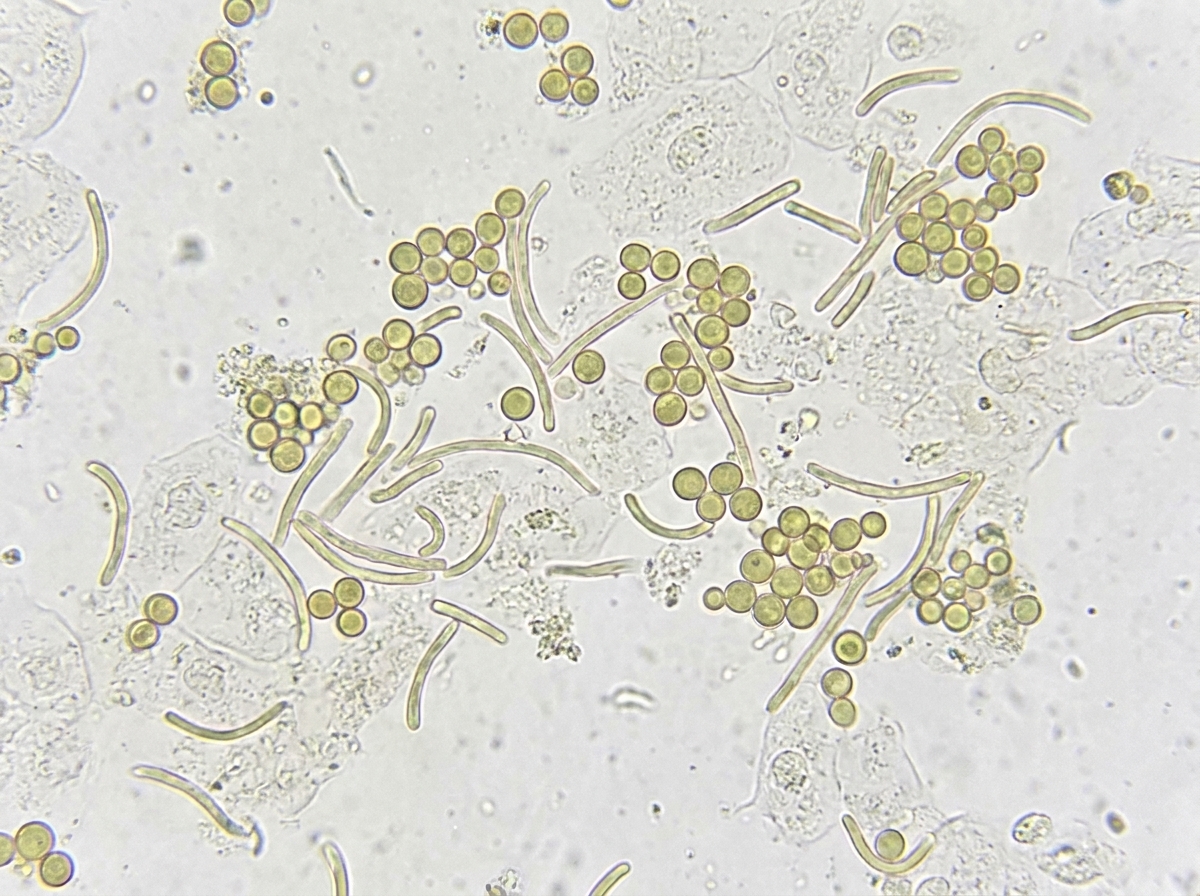
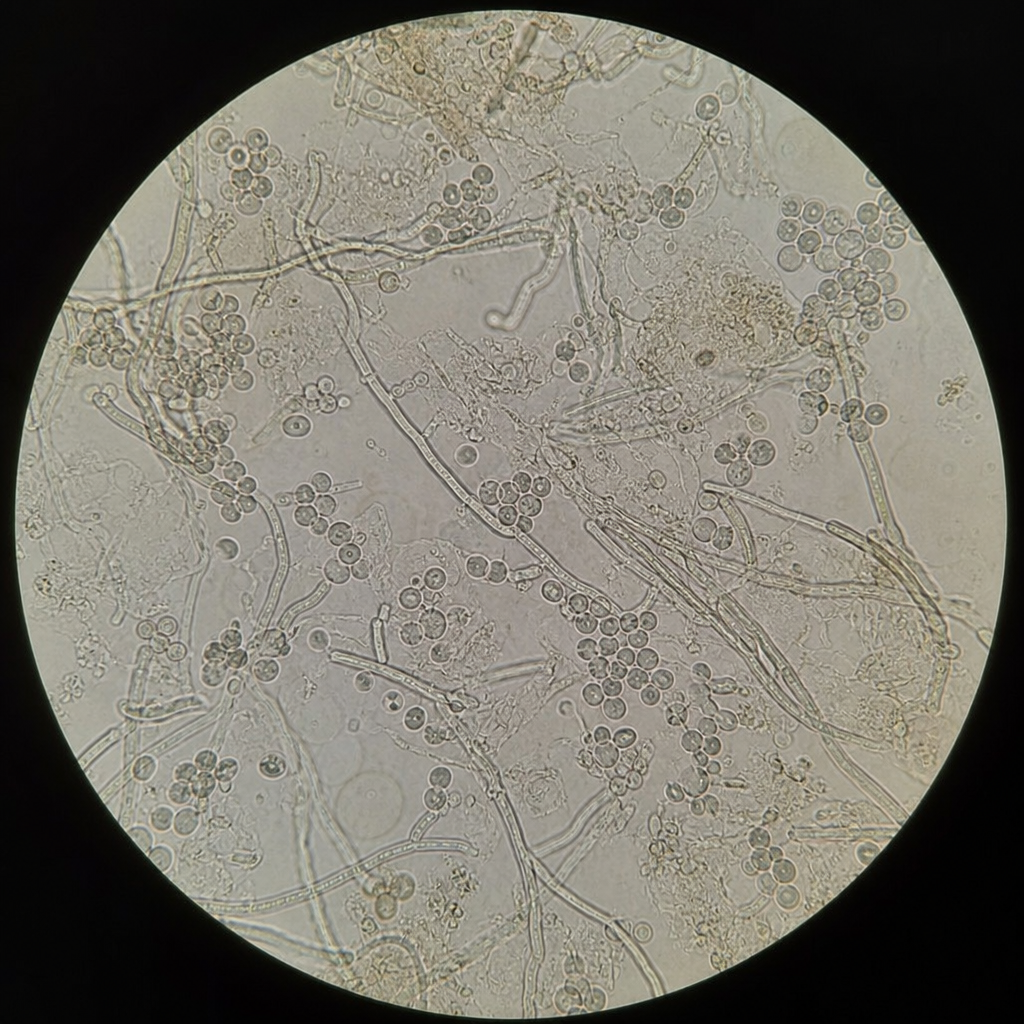
The given KOH mount of patient shows:
A 25-year-old construction worker presents with following skin lesions. All are true about the image shown except: (Recent NEET Pattern 2016-17)

All are true about the infection shown in the image EXCEPT:

The image shows a KOH mount suggestive of diagnosis of:
Practice by Chapter
Dermatophytoses
Practice Questions
Tinea Versicolor
Practice Questions
Candidiasis
Practice Questions
Onychomycosis
Practice Questions
Subcutaneous Mycoses
Practice Questions
Systemic Mycoses with Cutaneous Manifestations
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Mycetoma
Practice Questions
Tropical Fungal Infections
Practice Questions
Diagnosis of Fungal Infections
Practice Questions
Antifungal Therapy
Practice Questions
Preventive Strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app