
Fungal Skin Infections — MCQs

On this page
Tinea infection that presents with altered morphology after treatment with a topical steroid is known as:
Which of the following is NOT a treatment for Pityriasis versicolor?
A 40-year-old male presents with a rash over the groin characterized by demarcated peripheral scaling and central clearing. What is the most likely cause?
Vesicular lesions, indistinguishable from primary infection, which arise in other parts of the body of an allergic individual infected with Trichophyton are referred to as?
A patient with asymptomatic annular skin lesion as shown presents to OPD. Which investigation should be done?
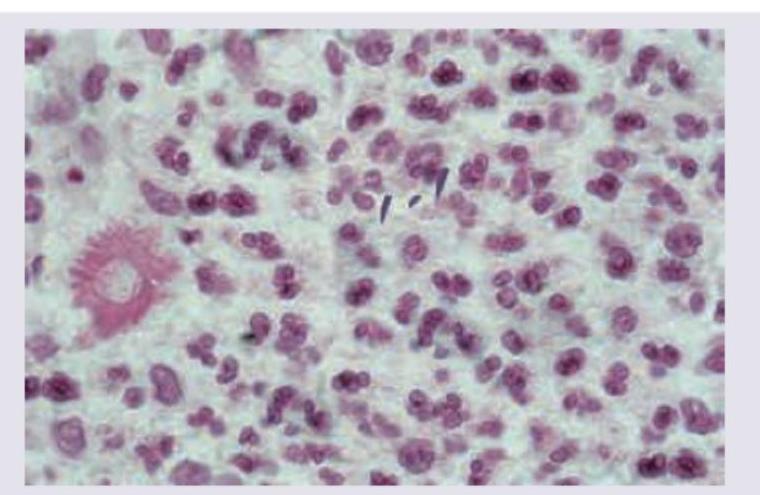
A carpenter presents with a nodule on dorsum of hand which ulcerates after few days and has not healed for last 2 months. Biopsy of lesion was performed and shown below. All are used in management of this condition except:
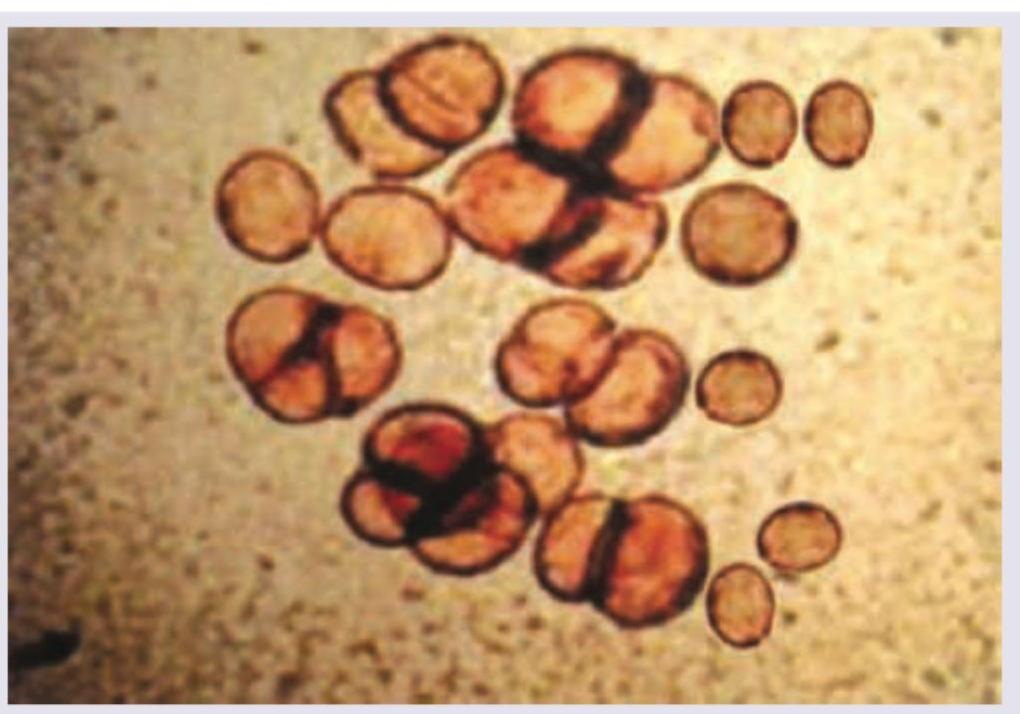
A female had a thorn prick 5 years ago. She presents with development of slowly growing $2 \times 2 \mathrm{~cm}$ verrucous lesion which on KOH mount shows the following image. Diagnosis is: (AIIMS Nov 2017)
All of the following statements regarding the image given below are true except:

Which of the following statements regarding the condition shown is false?

A patient presents with hypopigmented patches on the trunk. On examination, fine branny scaling is noted, and scratching the lesions enhances the scale (positive scratch sign). Wood-lamp examination reveals a yellow-green fluorescence. KOH preparation shows short hyphae and round spores. What is the most likely diagnosis?

Practice by Chapter
Dermatophytoses
Practice Questions
Tinea Versicolor
Practice Questions
Candidiasis
Practice Questions
Onychomycosis
Practice Questions
Subcutaneous Mycoses
Practice Questions
Systemic Mycoses with Cutaneous Manifestations
Practice Questions
Opportunistic Fungal Infections
Practice Questions
Mycetoma
Practice Questions
Tropical Fungal Infections
Practice Questions
Diagnosis of Fungal Infections
Practice Questions
Antifungal Therapy
Practice Questions
Preventive Strategies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app