
Enzymes — MCQs

On this page
What is true about ribozymes?
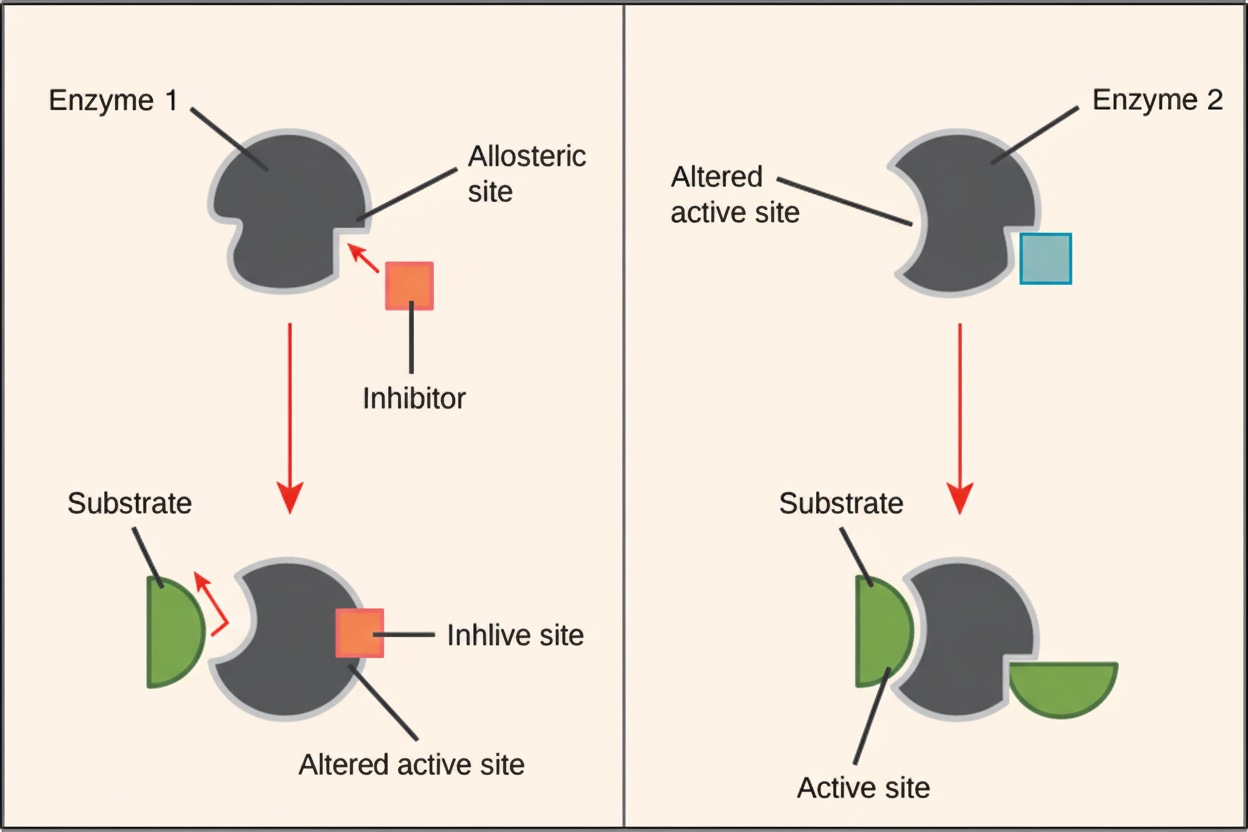
Regarding the regulation of enzyme activity as depicted in the diagram, which of the following statements is true?
Which of the following molecules can bind to the active site of an enzyme?
Which enzyme is activated by covalent phosphorylation?
Fumarase is classified as which type of enzyme?
Dehydrogenation of succinic acid to fumaric acid requires which of the following hydrogen carriers?
Which of the following is NOT a true statement about glucokinase?
Which of the following enzymes catalyzes the formation of AMP from two molecules of ADP?
Trypsin is a:
Isocitrate dehydrogenase is linked to which cofactor?
Practice by Chapter
Enzyme Classification and Nomenclature
Practice Questions
Enzyme Kinetics and Michaelis-Menten Equation
Practice Questions
Enzyme Inhibition: Competitive and Non-competitive
Practice Questions
Allosteric Regulation
Practice Questions
Coenzymes and Cofactors
Practice Questions
Isoenzymes and Clinical Significance
Practice Questions
Enzyme Regulation: Covalent Modification
Practice Questions
Enzyme Regulation: Zymogen Activation
Practice Questions
Enzyme Induction and Repression
Practice Questions
Ribozymes and Catalytic RNA
Practice Questions
Enzyme Diagnostic Applications
Practice Questions
Enzyme Therapy and Inhibitors as Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app