
Enzymes — MCQs

On this page
Which of the following is an allosteric inhibitor of pyruvate dehydrogenase?
What is the principal serum enzyme used in the clinical diagnosis of Wilson disease?
Lactate dehydrogenase is:
Which of the following covalent modifications does NOT regulate enzyme kinetics?
Which liver enzyme elevation suggests bile duct obstruction?
Molybdenum is a component of which enzyme?
Which of the following is most specific for cholestasis?
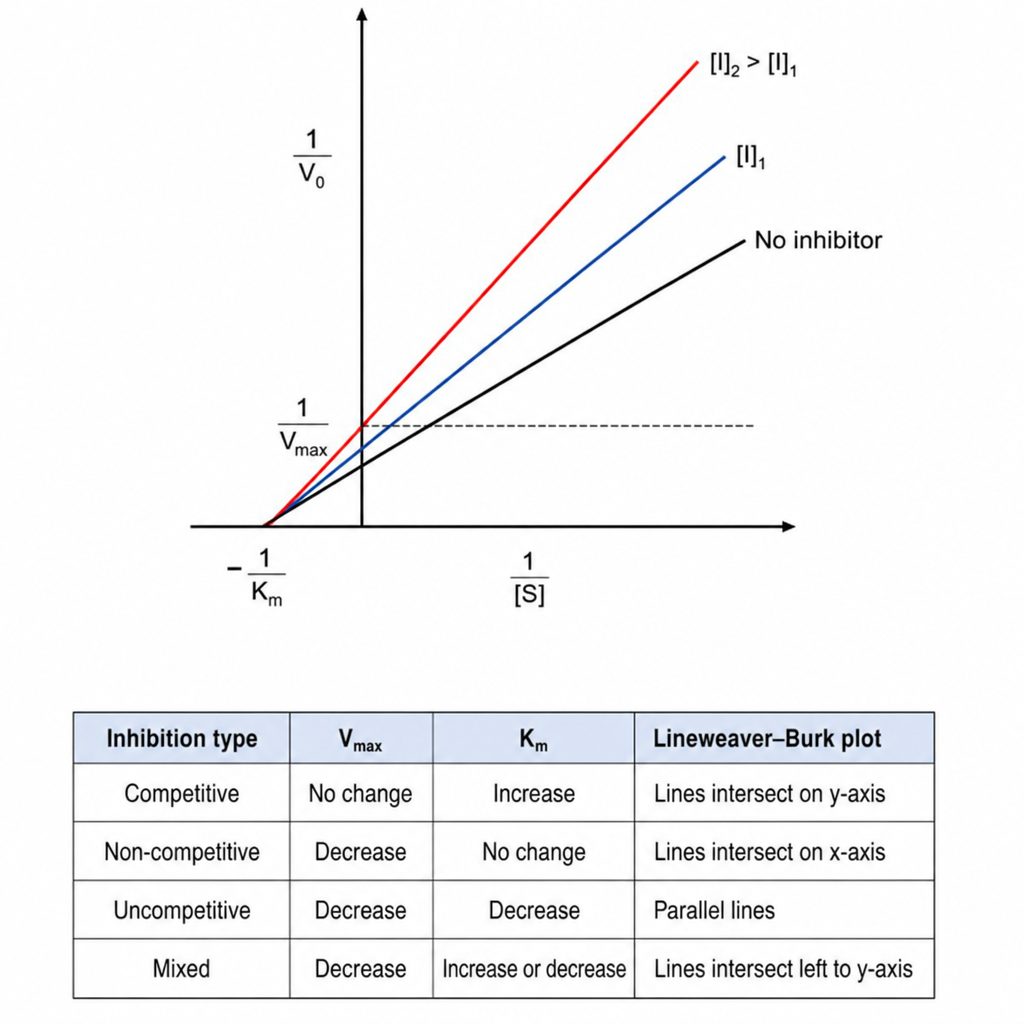
A patient took acetazolamide to combat altitude sickness. A graph depicting this medication's mechanism of enzyme inhibition is shown. What type of inhibitor is this medication?
Which enzyme serves as a marker for the pancreas?
Which of the following enzymes protects the brain from free radical injury?
Practice by Chapter
Enzyme Classification and Nomenclature
Practice Questions
Enzyme Kinetics and Michaelis-Menten Equation
Practice Questions
Enzyme Inhibition: Competitive and Non-competitive
Practice Questions
Allosteric Regulation
Practice Questions
Coenzymes and Cofactors
Practice Questions
Isoenzymes and Clinical Significance
Practice Questions
Enzyme Regulation: Covalent Modification
Practice Questions
Enzyme Regulation: Zymogen Activation
Practice Questions
Enzyme Induction and Repression
Practice Questions
Ribozymes and Catalytic RNA
Practice Questions
Enzyme Diagnostic Applications
Practice Questions
Enzyme Therapy and Inhibitors as Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app