
Enzymes — MCQs

On this page
The conversion of glutamate to glutamine is catalysed by which type of enzyme?
What is a marker of peroxisomes?
All of the following enzymes are increased in myocardial infarction, EXCEPT:
Flipped pattern of LDH is seen in which of the following conditions?
What is the cofactor for Glycogen phosphorylase in Glycogenolysis?
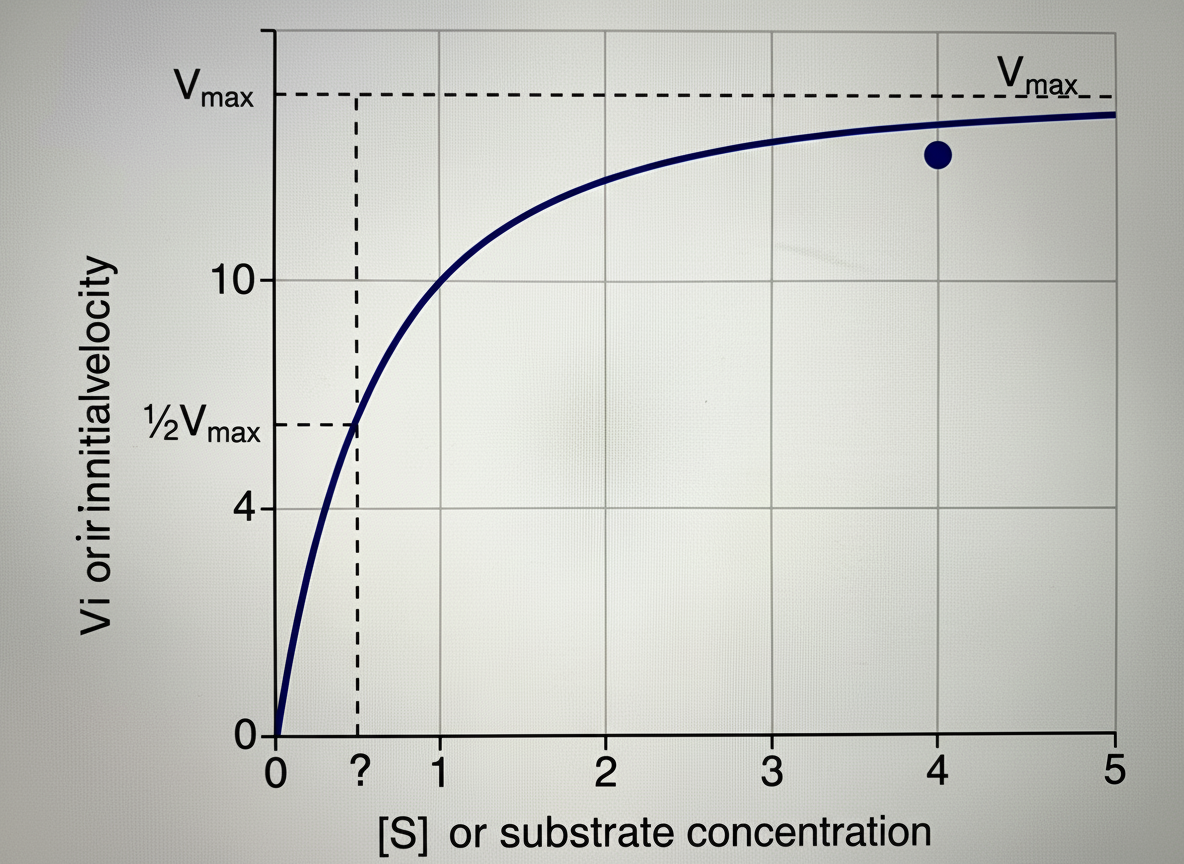
The provided graph illustrates the effect of substrate concentration on the initial velocity of an enzyme-catalyzed reaction. Identify the INCORRECT statement regarding this graph.
Which of the following statements is true about allosteric inhibition?
All of the following can be attributed to enzymatic catalysis, EXCEPT:
Which trace element is essential for the function of glutathione peroxidase?
Which of the following is an inhibitor of dihydrofolate reductase?
Practice by Chapter
Enzyme Classification and Nomenclature
Practice Questions
Enzyme Kinetics and Michaelis-Menten Equation
Practice Questions
Enzyme Inhibition: Competitive and Non-competitive
Practice Questions
Allosteric Regulation
Practice Questions
Coenzymes and Cofactors
Practice Questions
Isoenzymes and Clinical Significance
Practice Questions
Enzyme Regulation: Covalent Modification
Practice Questions
Enzyme Regulation: Zymogen Activation
Practice Questions
Enzyme Induction and Repression
Practice Questions
Ribozymes and Catalytic RNA
Practice Questions
Enzyme Diagnostic Applications
Practice Questions
Enzyme Therapy and Inhibitors as Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app