
Enzymes — MCQs

On this page
Which trace element is present in carbonic anhydrase?
Which enzyme is known as the 'suicidal enzyme'?
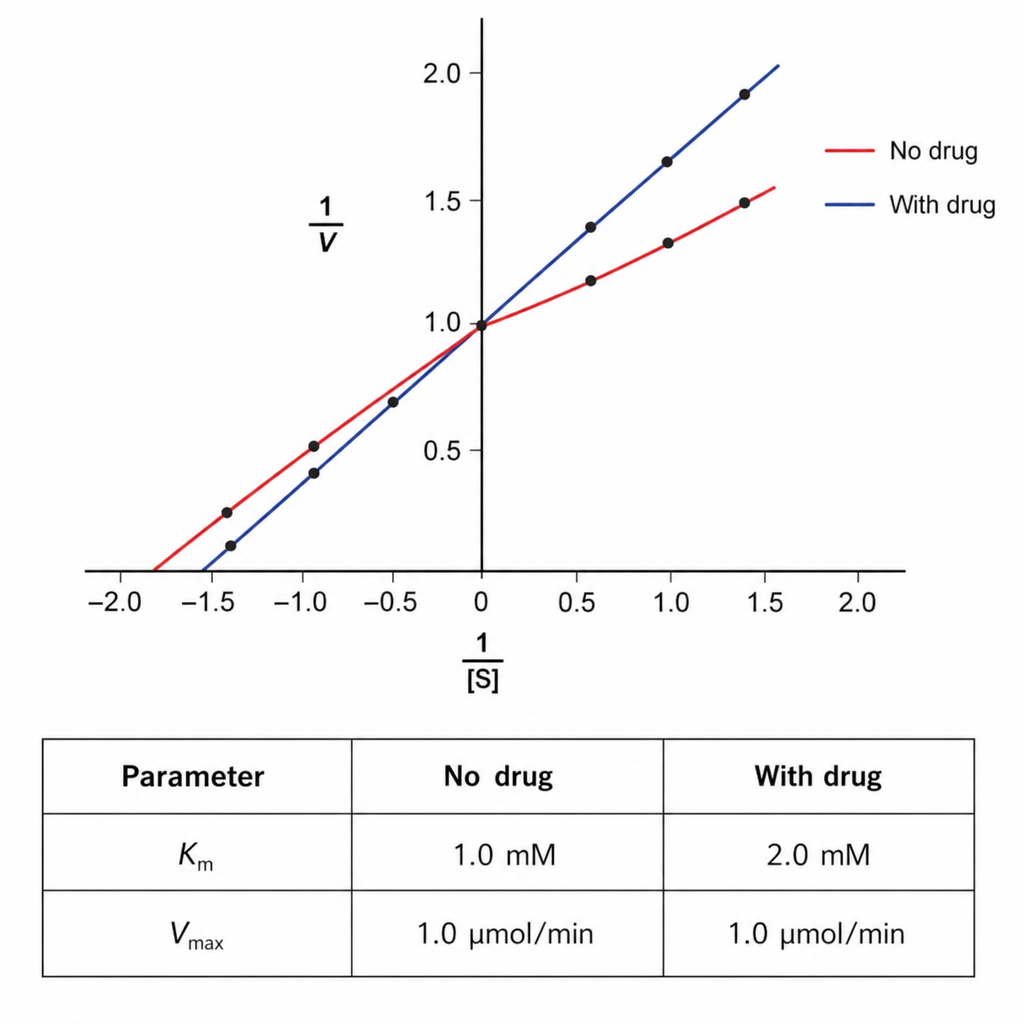
A 28-year-old female presents with fluctuating fatigue, drooping of her eyelids, difficulty swallowing, and slurred speech. The patient is given a drug that affects an enzyme's activity, and kinetic analysis of the enzyme-catalyzed reaction, in the presence and absence of the drug, is shown below. The effect of this medication can best be described by which set of terms below?
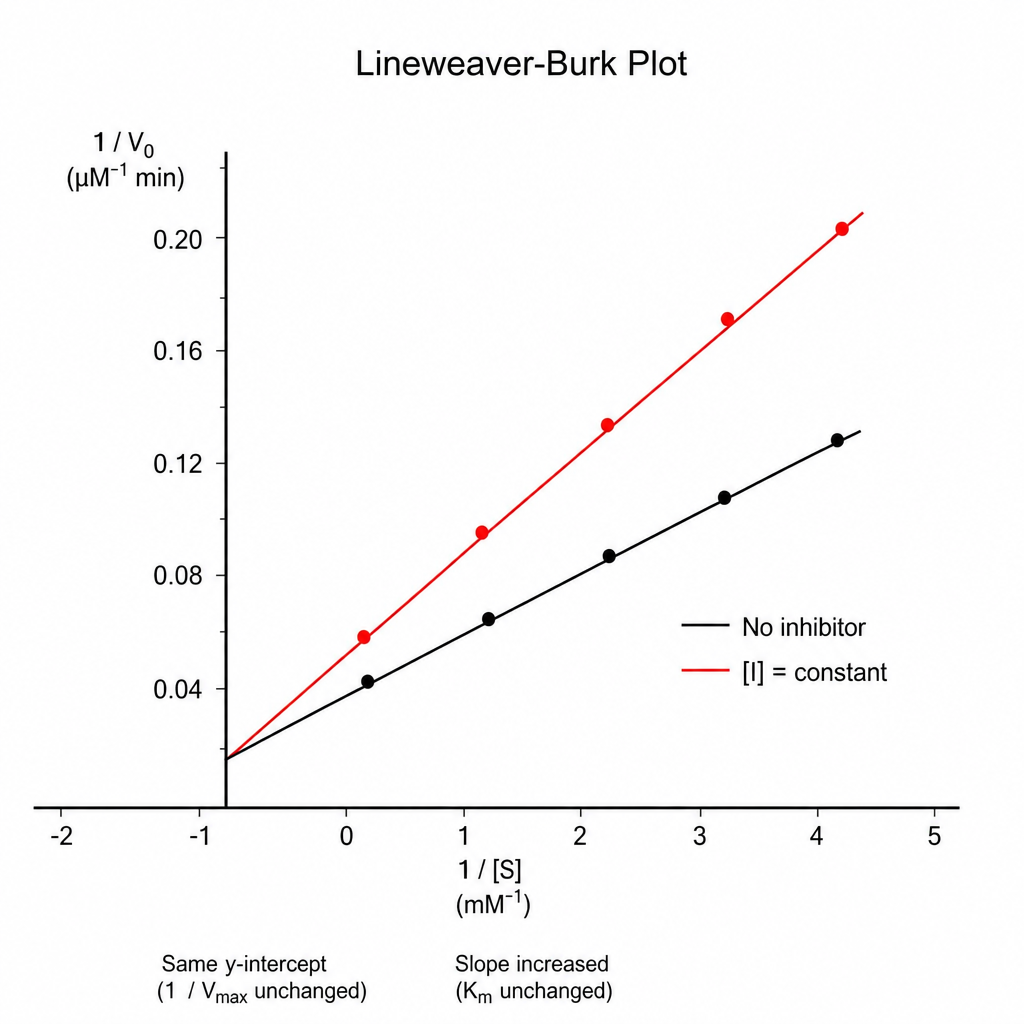
A kinetic analysis of the effect of a drug on an enzyme's activity was performed. Based on the results, into which of the following groups would the drug best fit?
Serum creatine kinase-3 (CK-3) is elevated in which of the following conditions?
Which of the following is a serum marker of rickets?
Copper is a constituent of which enzyme?
Which of the following is true regarding Nitric Oxide Synthase?
Which of the following is a selenium-containing enzyme?
NAD+ is reduced to NADH + H+ by dehydrogenases of all the following substrates, except?
Practice by Chapter
Enzyme Classification and Nomenclature
Practice Questions
Enzyme Kinetics and Michaelis-Menten Equation
Practice Questions
Enzyme Inhibition: Competitive and Non-competitive
Practice Questions
Allosteric Regulation
Practice Questions
Coenzymes and Cofactors
Practice Questions
Isoenzymes and Clinical Significance
Practice Questions
Enzyme Regulation: Covalent Modification
Practice Questions
Enzyme Regulation: Zymogen Activation
Practice Questions
Enzyme Induction and Repression
Practice Questions
Ribozymes and Catalytic RNA
Practice Questions
Enzyme Diagnostic Applications
Practice Questions
Enzyme Therapy and Inhibitors as Drugs
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app