
Trauma Anesthesia — MCQs

On this page
A patient suffered splenic rupture. His BP is 90/60 mmHg, PR 126/min and SpO2 92%. What is the induction agent of choice?
What is the best predictor in the Glasgow Coma Scale?
A patient with traumatic paraplegia due to injury of the thoracic cord at T3 level is observed to have a blood pressure of 210/120. What should be the initial management?
An RTA patient has received 4 units of packed RBCs within a few hours. Which of the following will be seen?
A soldier was buried in an avalanche and had multiple fractures in both legs. On evacuation and reaching base hospital, examination shows a heart rate = 60 / min, BP = 70/50 mm Hg. IV line access has failed on multiple occasions en route to the hospital. Hence the below shown route of administration of fluids was initiated on arrival to the hospital. Which site would enable fastest rate of administration?

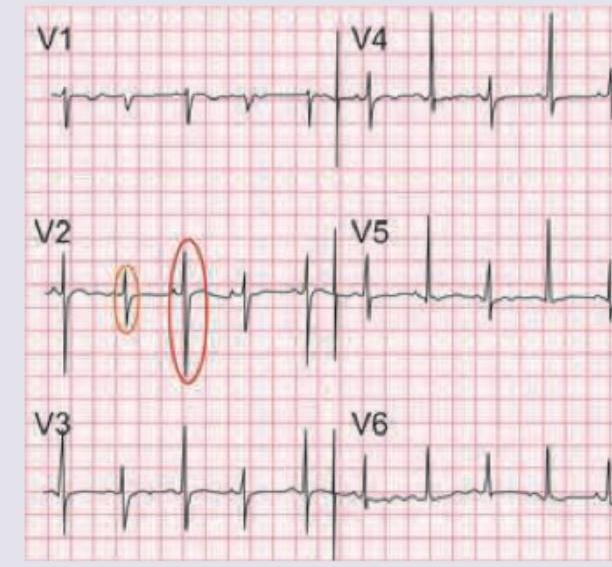
A 30-year-old male was brought to the ER after a car crash. On admission, pulse is weak with BP=80 / 60 mm Hg. ECG is shown below. Right heart catheter is placed. Which is the most consistent value with patient's diagnosis?
A case of trauma comes to the emergency. On examination there is evidence of head injury, BP is 90/60 mmHg, and pulse is 150/min. Which of the following anesthetic agent should be used for induction?
Massive transfusion is defined as transfusion of?
Which of the following anesthetics is contraindicated in head injury?
Practice by Chapter
Initial Assessment of Trauma Patients
Practice Questions
Airway Management in Trauma
Practice Questions
Shock and Resuscitation
Practice Questions
Massive Transfusion Protocol
Practice Questions
Traumatic Brain Injury Management
Practice Questions
Spinal Cord Injury Considerations
Practice Questions
Chest Trauma Management
Practice Questions
Abdominal Trauma Management
Practice Questions
Orthopedic Trauma Anesthesia
Practice Questions
Burns Management
Practice Questions
Pediatric Trauma Anesthesia
Practice Questions
Damage Control Surgery Anesthesia
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app