
General Anesthesia — MCQs

On this page
Which inhalational anesthetic agent has the lowest blood-gas coefficient?
Arrhythmias are most common when adrenaline is used with which of the following inhaled anesthetics?
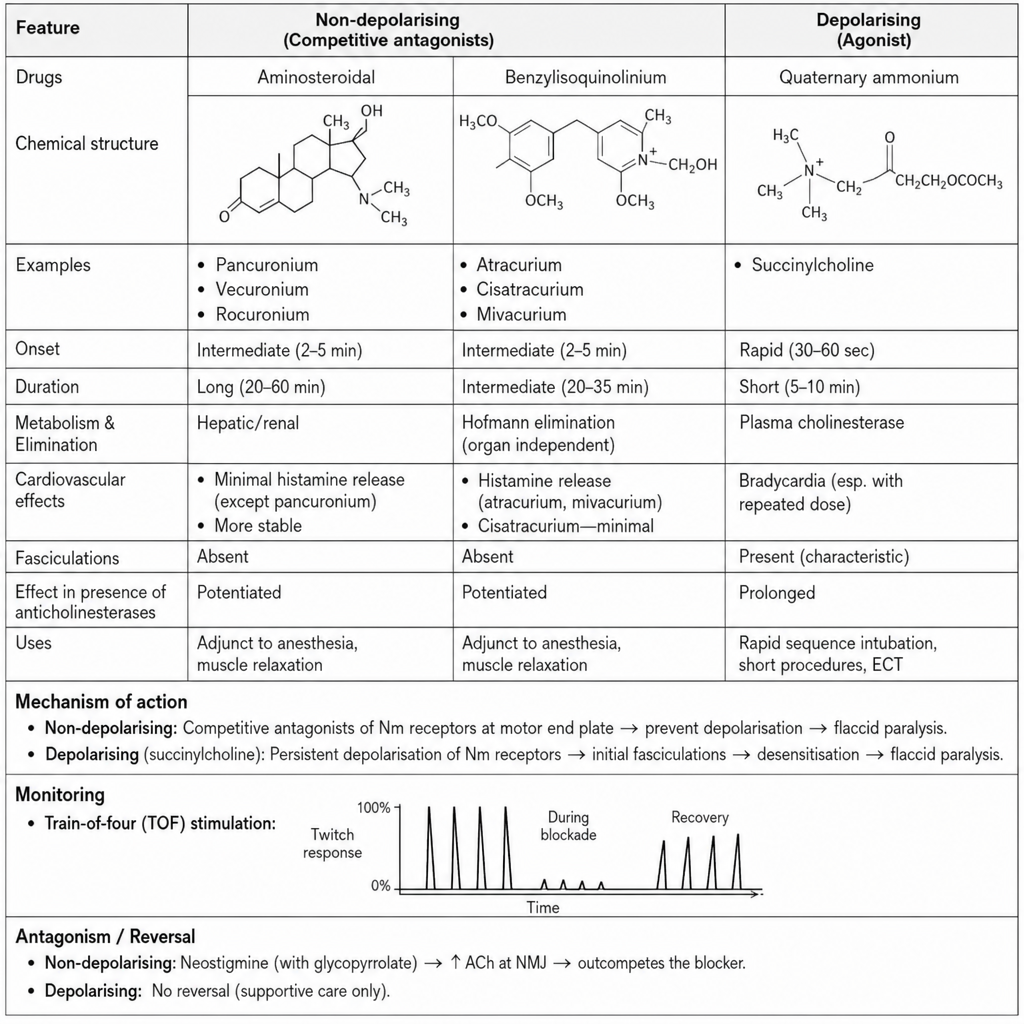
Which of the following statements regarding Non-Depolarizing Muscle Relaxants is FALSE?
Which of the following statements regarding neuromuscular blockers are true?
The rate at which the alveolar concentration of an anesthetic approaches inspired concentration is a function of all except?
Polygelin content is found in which of the following fluids?
Which of the following is the fastest acting anesthetic agent?
Which of the following solutions is a colloid?
Which intravenous anesthetic agent produces a cocaine-like effect on the cardiovascular system?
Which of the following drugs has caused hyperkalemia leading to cardiac arrest in patients with neurological disorders?
Practice by Chapter
History of Anesthesia
Practice Questions
Preoperative Evaluation
Practice Questions
Pharmacology of Inhalational Anesthetics
Practice Questions
Pharmacology of Intravenous Anesthetics
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Airway Management
Practice Questions
Endotracheal Intubation
Practice Questions
Difficult Airway Algorithms
Practice Questions
Intraoperative Monitoring
Practice Questions
Depth of Anesthesia Monitoring
Practice Questions
Emergence from Anesthesia
Practice Questions
Postoperative Care
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app