
General Anesthesia — MCQs

On this page
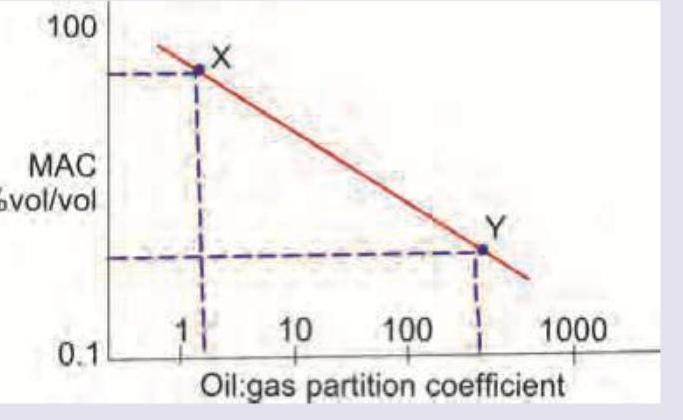
Which is correct about the anesthetic drugs X and Y in the image shown? (Recent NEET Pattern 2016-17)
The commonly used muscle relaxant with quickest onset of action and spontaneous recovery is :
Muscle relaxant ideal for rapid intubation and short procedures is:
Which one of the following is a Nephrotoxic anaesthetic agent ?
A patient with mild to moderate renal failure requires reversal of muscle relaxation induced by vecuronium. Which of the following drugs is appropriate for this purpose?
Arrange the following anesthetic agents based on their potency Nitrous oxide Halothane Isoflurane Methoxyflurane
Which of the following drugs is used for hypotensive anesthesia:
Which of the following inhalational anaesthetic agent can cause hepatitis on repeated use?
Which of the following is the most suitable anesthetic agent for use in dogs?
Dose of ketamine by IM route is (in mg/kg) –
Practice by Chapter
History of Anesthesia
Practice Questions
Preoperative Evaluation
Practice Questions
Pharmacology of Inhalational Anesthetics
Practice Questions
Pharmacology of Intravenous Anesthetics
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Airway Management
Practice Questions
Endotracheal Intubation
Practice Questions
Difficult Airway Algorithms
Practice Questions
Intraoperative Monitoring
Practice Questions
Depth of Anesthesia Monitoring
Practice Questions
Emergence from Anesthesia
Practice Questions
Postoperative Care
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app