
General Anesthesia — MCQs

On this page
Which of the following are characteristics of Remifentanyl?
Which of the following induction agents produces cardiac stability?
Ketamine can be administered by all of the following routes except?
Postoperative muscle ache is commonly caused by which of the following agents?
What is the role of egg lecithin in propofol formulation?
Which of the following inhalation agents has a blood-gas partition coefficient similar to nitrous oxide?
A 35 y/o asthmatic patient is scheduled for a minor surgical procedure. Which induction agent and muscle relaxant combination is safest for this patient?
A patient undergoing surgery receives a muscle relaxant and soon develops flushing and rashes over the neck and anterior chest. Which of the following muscle relaxants is most commonly associated with this reaction?
A 50-year-old male patient underwent lower abdominal surgery under general anaesthesia. Vecuronium was administered as a muscle relaxant during the procedure. At the end of the surgery, which of the following is the most appropriate agent to reverse the effects of vecuronium?
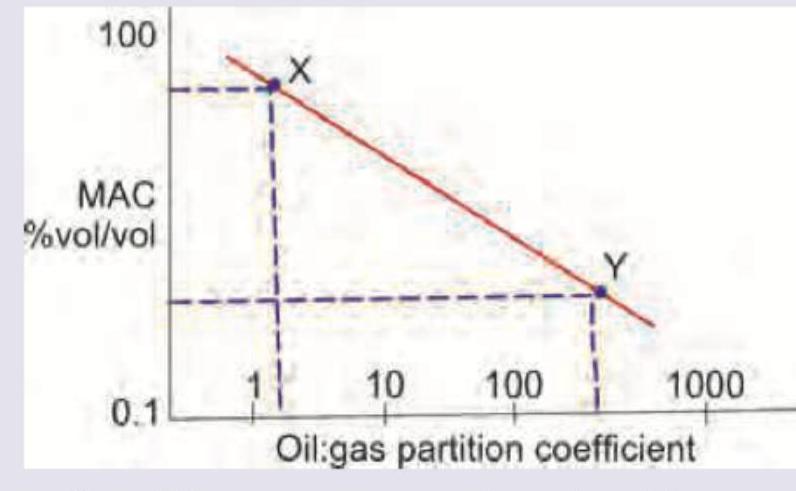
Which is correct about the anesthetic drugs X and Y respectively?
Practice by Chapter
History of Anesthesia
Practice Questions
Preoperative Evaluation
Practice Questions
Pharmacology of Inhalational Anesthetics
Practice Questions
Pharmacology of Intravenous Anesthetics
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Airway Management
Practice Questions
Endotracheal Intubation
Practice Questions
Difficult Airway Algorithms
Practice Questions
Intraoperative Monitoring
Practice Questions
Depth of Anesthesia Monitoring
Practice Questions
Emergence from Anesthesia
Practice Questions
Postoperative Care
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app