
General Anesthesia — MCQs

On this page
What is true about ketamine?
Thiopentone is contraindicated in which of the following conditions?
Which of the following is a known effect of suxamethonium?
A 21-year-old woman with a history of hypersensitivity to neostigmine is scheduled for an elective cesarean section under general anesthesia. Which muscle relaxant is the best choice for this patient?
Nitrous oxide is contraindicated in which of the following conditions?
Pain during injection occurs with all anesthetic agents listed below except?
Which volatile anesthetic agent causes the most renal toxicity?
A 60-year-old man undergoing an inguinal hernia repair is induced with propofol. Which of the following is most likely to be observed?
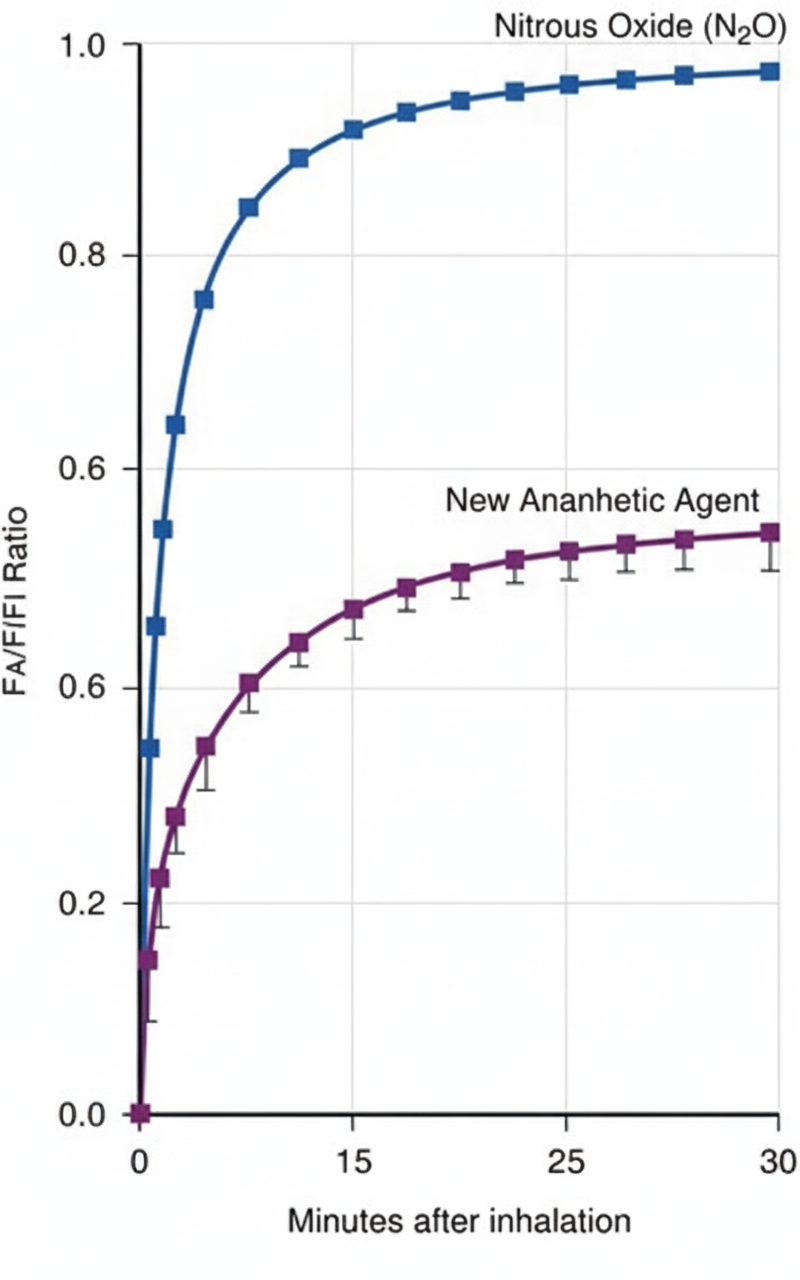
The FA/FI ratio (alveolar to inspired concentration) of a new anesthetic agent is plotted against time after inhalation on the graph below. A similar curve for nitrous oxide is also shown. Assuming all other determinants of uptake are held constant, which of the following best describes the properties of the new anesthetic compared to nitrous oxide?
Which of the following muscle relaxants is free of cardiovascular effects over the entire clinical dose range?
Practice by Chapter
History of Anesthesia
Practice Questions
Preoperative Evaluation
Practice Questions
Pharmacology of Inhalational Anesthetics
Practice Questions
Pharmacology of Intravenous Anesthetics
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Airway Management
Practice Questions
Endotracheal Intubation
Practice Questions
Difficult Airway Algorithms
Practice Questions
Intraoperative Monitoring
Practice Questions
Depth of Anesthesia Monitoring
Practice Questions
Emergence from Anesthesia
Practice Questions
Postoperative Care
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app