
General Anesthesia — MCQs

On this page
Which of the following intravenous agents is commonly used for outpatient procedures?
A 40-year-old female is scheduled for parotid surgery and is administered general Anaesthesia. Approximately 10 minutes into the procedure, the following findings are noted: - Rise in end-tidal CO2 (EtCO2) - Temperature: 104°F (40°C) - Heart rate: 150 bpm - Blood pressure: 180/110 mmHg What is the most likely diagnosis?
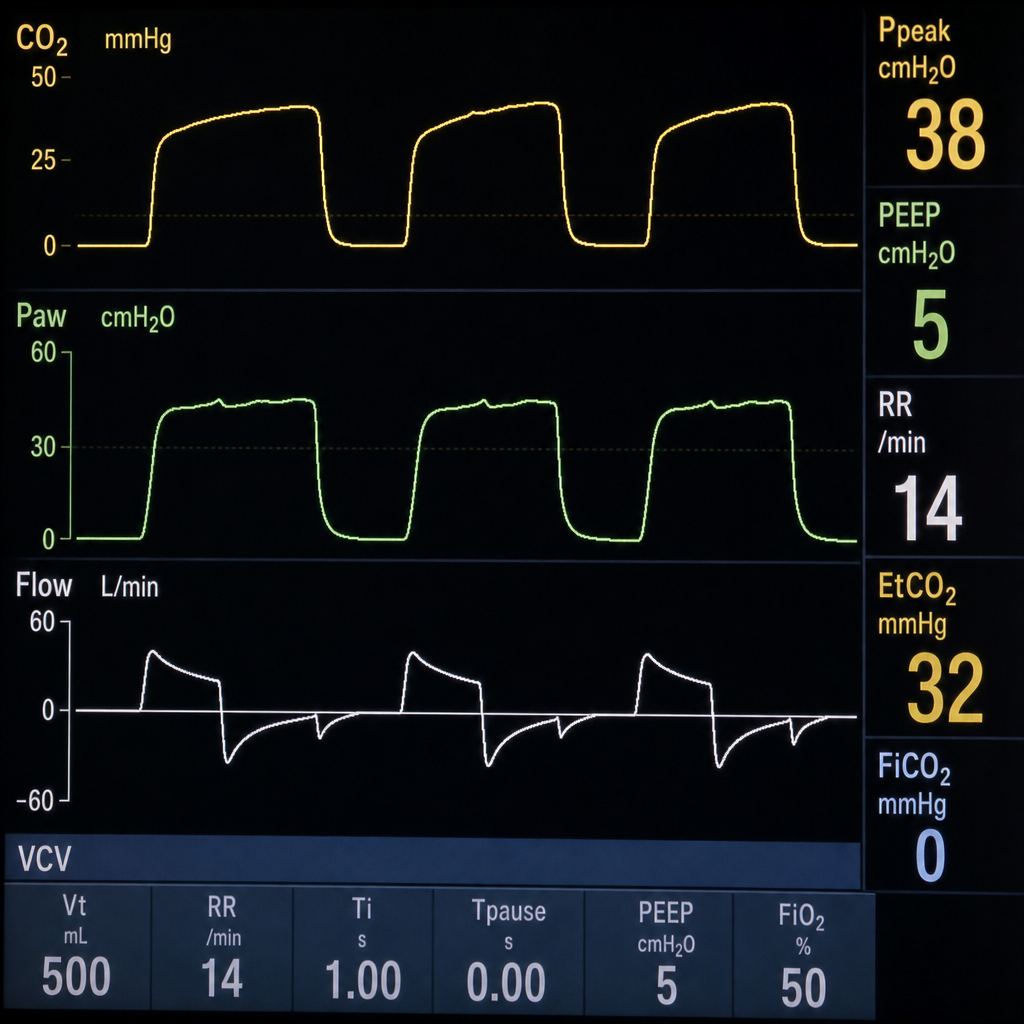
A 34-year-old asthmatic male undergoes elective laparoscopic cholecystectomy under general anesthesia with endotracheal intubation. Fifteen minutes after induction, the ventilator alarm sounds for high peak airway pressure. The anesthesiologist notes the waveform shown on the capnograph monitor (Image 1). What is the most likely cause of this capnographic pattern?
Diffusion hypoxia is seen with which drug?
All of the following are modes to decrease pain on injection caused by propofol except?
Which of the following statements about nitrous oxide is FALSE?
Which of the following drugs are known to be hepatotoxic?
Non-depolarizing neuromuscular blockade is potentiated by which of the following conditions or medications?
Which of the following muscle relaxants is contraindicated in muscular dystrophy?
A 35-year-old patient is given excessive intravenous Benzodiazepine. She suddenly becomes agitated, combative, and exhibits involuntary movements. The anesthesiologist determines that she is having a reaction to the drug which has been given in excess. What is the next step in management?
Practice by Chapter
History of Anesthesia
Practice Questions
Preoperative Evaluation
Practice Questions
Pharmacology of Inhalational Anesthetics
Practice Questions
Pharmacology of Intravenous Anesthetics
Practice Questions
Neuromuscular Blocking Agents
Practice Questions
Airway Management
Practice Questions
Endotracheal Intubation
Practice Questions
Difficult Airway Algorithms
Practice Questions
Intraoperative Monitoring
Practice Questions
Depth of Anesthesia Monitoring
Practice Questions
Emergence from Anesthesia
Practice Questions
Postoperative Care
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app