
Critical Care Medicine — MCQs

On this page
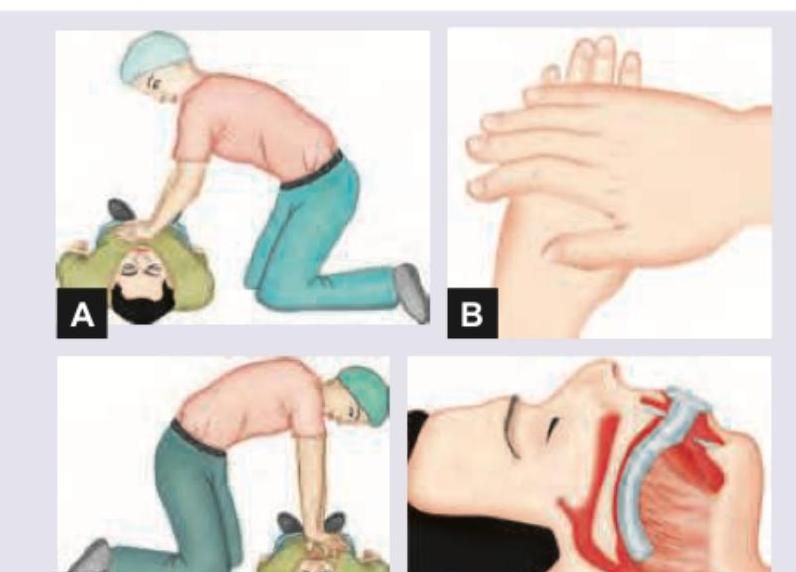
In CPR, where are chest compressions performed?
A 74-year-old man with a history of myocardial infarction 3 years prior underwent elective repair of an abdominal aortic aneurysm. On the first postoperative day in the ICU, he is hypotensive and receiving dobutamine. What is the best method of physiologic monitoring necessary for this patient?
What is the drug of choice for sedation of a patient in the ICU?
A patient is in ICU and there is a failed attempt of subclavian catheterization. Shortly after, BP drops and the pulse rises. What is the diagnosis?
According to the American Heart Association (AHA), what is the 6th link added to the chain of survival?
Patient in hospital was given IVF and patient develops hyperchloremic metabolic acidosis. Which fluid will cause this?
A 65-year-old patient is on mechanical ventilation for acute respiratory distress syndrome (ARDS). Suddenly, the patient becomes hypotensive, tachycardic, and shows absent breath sounds on the left side with tracheal deviation to the right. What is the most common cause of this in patients receiving mechanical ventilation?
Which of the following is the correct technique of giving CPR?
A comatose patient after sustaining severe head injury has been admitted to the neurosurgical ICU. Which of the following parameters should ideally be maintained in this patient? 1. pCO2 = 4.5 - 5.0 kPa (33-38 mm Hg) 2. MAP = 80 - 90 mm of Hg 3. pO2 > 11 kPa (> 80 mm Hg) 4. Na+ < 130 meq/L
Patient of pneumonia on ventilator with wt. 50 kg. RR 14/min, bicarbonate - 18, pH 7.3, pCO2 48 mmHg, pO2 110 mmHg, PEEP 12 cm H2O, tidal volume 420 mL, SpO2 - 100% with FiO2 90%. What is next step in management?
Practice by Chapter
Applied Respiratory Physiology
Practice Questions
Mechanical Ventilation Principles
Practice Questions
Ventilator Management Strategies
Practice Questions
Acute Respiratory Distress Syndrome
Practice Questions
Shock: Classification and Management
Practice Questions
Hemodynamic Monitoring in ICU
Practice Questions
Acid-Base Disorders
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Sedation and Analgesia in ICU
Practice Questions
Neurocritical Care
Practice Questions
Renal Replacement Therapy
Practice Questions
Nutrition in Critical Illness
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app