
Neuroanatomy — MCQs

On this page
What is the blood supply of the great toe?
Which drug is contraindicated for use along with local anaesthetics?
Which of the following types of leukemia almost never develops after radiation exposure?
What is the most common nerve involved in cavernous sinus thrombosis?
A fixed firm belief that the patient has subjective certainty is called as?
Which of the following is an example of a traction epiphysis?
Which of the following structures is most likely to be compressed by an aneurysm of the posterior communicating artery?
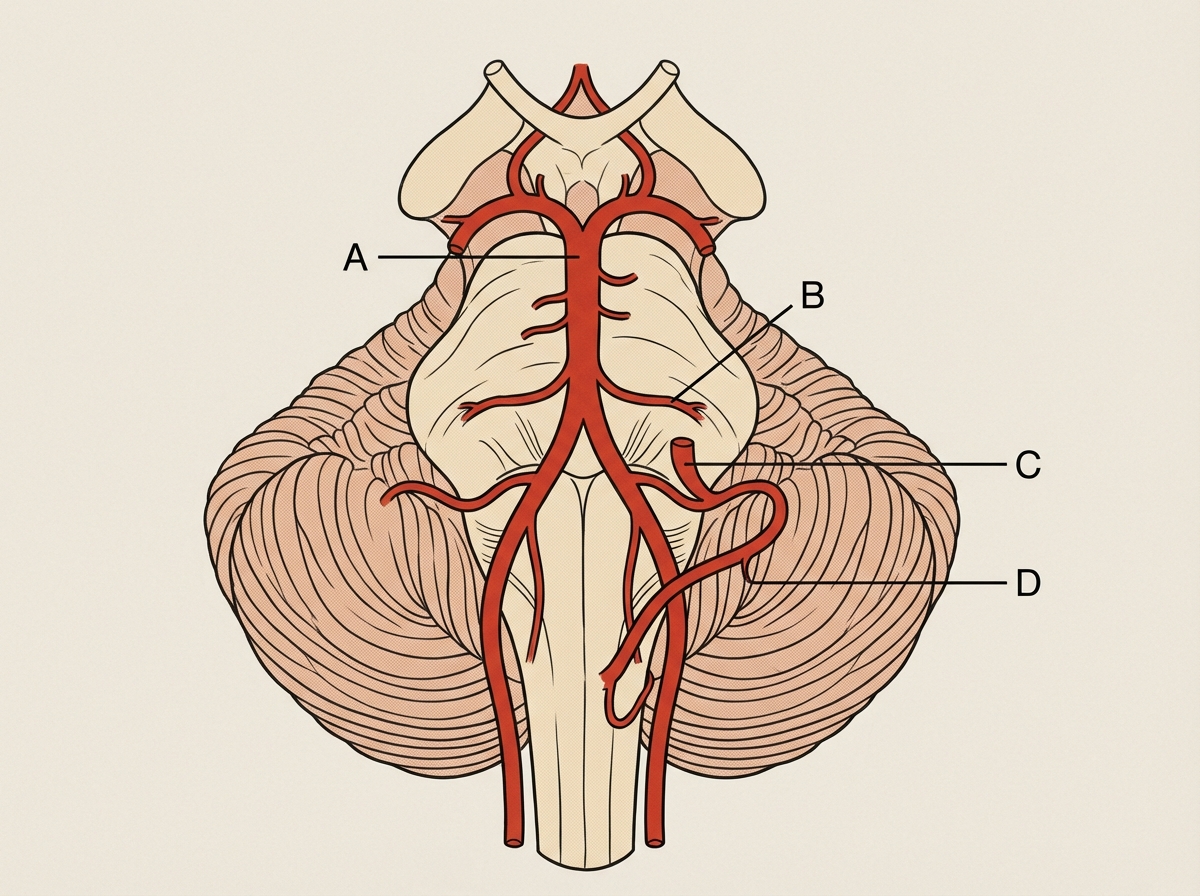
Which artery is involved in Wallenberg syndrome?
Which of the following is a hallmark of acute inflammation?
What is a ganglion?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app