
Neuroanatomy — MCQs

On this page
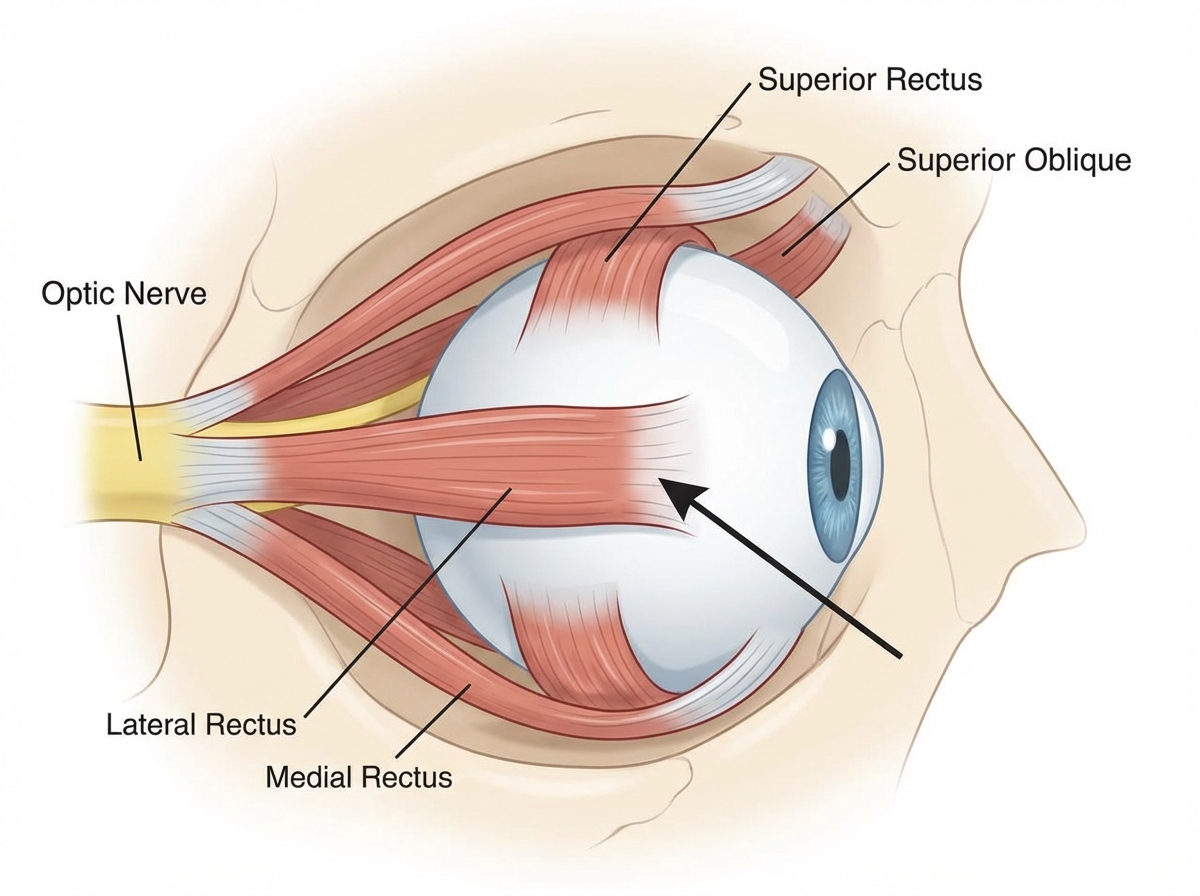
The cranial nerve nucleus supplying the marked muscle lies at the level of:
Which of the following is not included in Jones major criteria for Rheumatic Fever?
Which of the following immunoglobulins does not fix complement?
What is the most common cause of delayed umbilical cord separation?
Transection of the anterolateral spinothalamic tract results in what kind of sensory deficit?
Which of the following are components of the cytoskeleton?
Which type of Ehlers-Danlos syndrome is considered the catastrophic variant?
Which of the following are affected in graft versus host reaction?
What is the earliest physical sign of sexual maturation in females?
In which nucleus does the dorsal column relay occur?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app